TL;DR: A 2026 service-mapping study in BJPsych Bulletin found that community forensic mental health services (CFMHS), specialist teams for people with mental disorder and serious risk histories, still vary widely across England in structure, referral access, staffing, and crisis coverage.
Key Findings
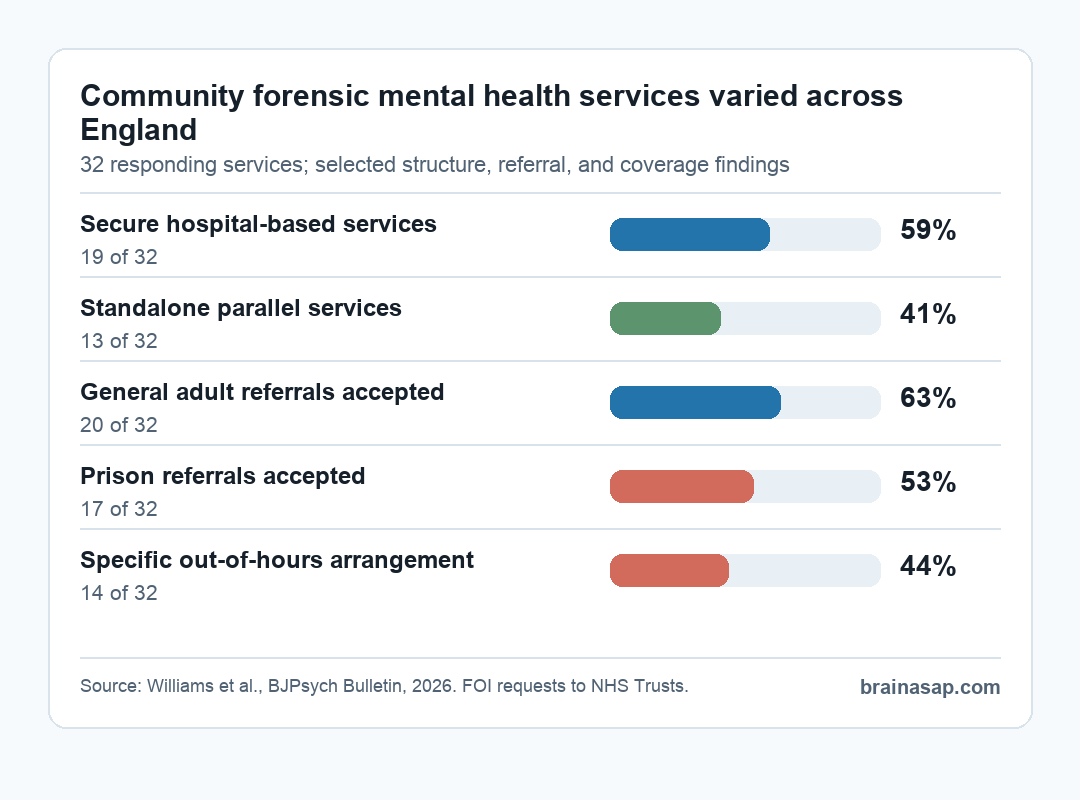
- 32 services responded: Researchers received data from 32 CFMHS after sending Freedom of Information requests to 50 NHS Trusts in England.
- Service models split: 59% were part of secure hospital-based services, while 41% were standalone teams working in parallel with general mental-health services.
- Referral routes varied: All services accepted referrals from forensic in-patient services, but only 63% accepted general adult community referrals and 53% accepted prison referrals.
- Crisis coverage was uneven: 44% reported a specific out-of-hours arrangement; the rest operated as weekday daytime services.
- Psychology was common: 94% reported psychological interventions, although treatment modalities differed across the services that gave details.
Source: BJPsych Bulletin, 2026.
The hard part is the handoff. People leaving secure psychiatric care may need recovery support, risk planning, medication oversight, housing coordination, and a route back into ordinary community life.
These teams also coordinate with courts, prisons, community teams, crisis systems, and public-safety agencies. The Williams study maps how uneven that junction still looks in practice.
Researchers sent Freedom of Information requests to 50 NHS Trusts in England. The responses described 32 community forensic services, including team structure, staffing, referral criteria, legal-status policies, treatment provision, and out-of-hours arrangements.
This was not a patient-outcome trial. It was a service-configuration audit, so the main result is about system design rather than symptom change.
Forensic Mental Health Teams Did Not Fit One Simple Model
The study found a broad split between two service structures. 19 services were described as part of secure hospital-based services, while 13 services were standalone teams working alongside general services.
That split is useful, but researchers emphasized that it still oversimplifies the real landscape.
Several details made the service map messier than a two-category label:
- Secure-hospital extensions: Some teams mainly followed patients after secure in-patient care and kept close operational links to hospital units.
- Standalone parallel teams: Other services operated separately from general adult mental-health teams while still receiving referrals from broader clinical settings.
- Mixed interfaces: Referral routes, crisis arrangements, and legal-status policies differed enough that the same label could hide different day-to-day functions.
That variation has clinical consequences because CFMHS are meant to coordinate risk management, recovery, and least-restrictive care.
If service boundaries differ sharply by region, clinicians and referrers may not know whether a patient should be managed by forensic specialists, general adult services, prison mental-health teams, or a shared-care arrangement.
Referral Access Was Broader for Some Patients Than Others
Every service accepted referrals from in-patient forensic services. Beyond that, access was less consistent.
20 services accepted referrals from general adult community mental-health teams, 18 accepted referrals from non-secure in-patient services, and 17 accepted referrals for people in prison.
The referral findings point to three practical access questions:
- Hospital discharge: Does the service automatically accept people leaving secure hospital, or does it require a separate referral decision?
- Community risk support: Can general adult teams request forensic input before a person reaches a secure-hospital threshold?
- Prison transition: Can prison mental-health teams directly connect people with specialist community forensic support before release?
The prison route is especially important. The study authors noted that serious mental illness after prison release is already a known risk period for reoffending and reincarceration.
If only about half of CFMHS accept prison referrals, then some regions may have a weaker specialist bridge between custody, mental-health care, and community risk management.
Staffing Was Multidisciplinary, But Not Uniform
Most services had the core professions readers would expect in forensic psychiatric care. Psychiatrists and psychologists were each represented in 94% of services, and community psychiatric nurses were represented in 97%.
Social workers appeared in 78%, and occupational therapists in 69%.
Staffing variation showed up around additional professional roles and service intensity:
- Assistant psychologists: 63% of services reported this role, with a higher proportion in secure hospital-based services.
- Peer support: 22% of services reported workers with lived experience.
- Employment support: 22% included education, training, and employment workers.
- Caseload targets: Where reported, care-coordinator targets usually ranged from 10 to 20 patients per full-time staff member, with one outlier at 70.
Those differences do not automatically mean one service is better than another. They do mean that a patient described as under a CFMHS may receive a different mix of psychiatric oversight, psychology, nursing, social-work input, occupational therapy, and recovery support depending on geography and local commissioning.
Psychological Treatment and Crisis Coverage Also Varied
Psychological interventions were reported by 30 services, or 94%. Among the 17 services that provided details on treatment modality, dialectical behaviour therapy was reported by 71%, cognitive-behavioural therapy by 65%, schema therapy by 47%, and cognitive analytic therapy by 35%.
Out-of-hours coverage was more limited. 14 services reported a specific arrangement for support outside normal hours.
The remaining services operated between 09:00 and 17:00, Monday to Friday. Some teams used their own on-call cover, while others relied on Trust-wide crisis or out-of-hours systems.
For high-risk community psychiatric care, that distinction is not a small operational detail. A daytime-only specialist team may still provide good planned care, but crisis support then depends on how well general crisis teams, forensic clinicians, in-patient units, and justice agencies share information after hours.
Why Standardization Is Still a Research Problem
The study’s main service-level message is direct: variation makes evaluation harder. If CFMHS differ in referral routes, staffing, treatment role, legal-status management, and crisis coverage, then national standards and outcome studies have to define which model they are evaluating.
Researchers also reported important limits. The survey was exploratory, responses came from 80% of Trusts, and staffing numbers were not fully adjusted for caseload size or catchment population.
The study also did not collect detailed commissioning or funding arrangements, which likely shape service design.
The service lesson is not that every CFMHS should look identical. Local need is still relevant.
The evidence instead points to a narrower operational problem: when specialist forensic community care is defined differently across regions, patients, referrers, and researchers may all be using the same service label for different systems.
Citation: DOI: 10.1192/bjb.2026.10236. Williams et al. Community forensic mental health services in England: mapping provision, structure and function. BJPsych Bulletin. 2026.
Study Design: Exploratory service-mapping study using Freedom of Information requests to NHS Trusts in England.
Sample Size: 32 community forensic mental health services provided data after requests were sent to 50 Trusts.
Key Statistic: 59% of responding services were secure hospital-based, 41% were standalone parallel teams, and 44% reported specific out-of-hours arrangements.
Caveat: Service responses describe structure and provision, not patient outcomes or comparative effectiveness.