TL;DR: A 2026 systematic review posted on medRxiv found that transcranial direct current stimulation (tDCS), a weak noninvasive brain-stimulation method, added to cognitive training produced a small short-term cognitive benefit across 27 trials, but the effect faded at follow-up and the evidence certainty was very low.
Key Findings
- 27 controlled studies: The meta-analysis included 1,012 participants with cognitive impairment linked to stroke, Alzheimer’s disease, mild cognitive impairment, HIV, multiple sclerosis, or primary progressive aphasia.
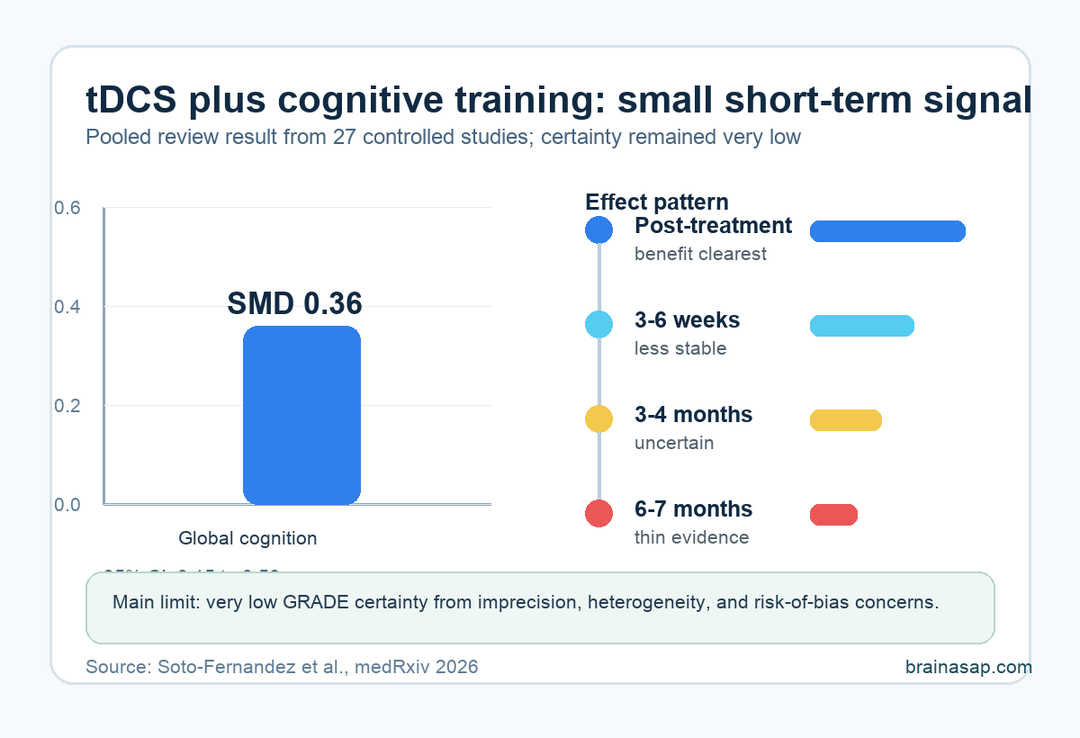
- Small global cognitive effect: Adding tDCS to cognitive training improved global cognitive performance by SMD 0.36 versus cognitive training alone.
- Immediate benefit only: The pooled cognitive advantage was strongest right after treatment and became less stable across later follow-up windows.
- Functional gains were narrower: Daily-function outcomes looked most favorable in post-stroke cognitive impairment, while other conditions had sparse or uncertain results.
- Very low certainty: GRADE ratings were pulled down by imprecision, study heterogeneity, and risk-of-bias concerns, so the review does not establish a ready clinical protocol.
Source: medRxiv preprint (2026) | Soto-Fernandez et al.
Cognitive training asks patients to practice memory, attention, language, or executive-control tasks. Transcranial direct current stimulation tries to nudge cortical excitability while that training is happening, usually by sending a low electrical current through scalp electrodes.
The practical question is simple: does adding stimulation make rehabilitation work better than the same cognitive practice alone?
tDCS Added a Small Short-Term Cognitive Gain
The review searched randomized and controlled trials in adults with mild or moderate cognitive impairment. Across the quantitative set, 27 studies contributed data, and 23 studies with 1,012 participants fed the main global cognitive-performance estimate.
The pooled effect favored combined stimulation plus training. The standardized mean difference was 0.36, with a 95% confidence interval from 0.15 to 0.56. That estimate is a small effect, not a dramatic cognitive restoration.
The comparison matters because the control arm was not no treatment. The question was whether electrical stimulation added something beyond structured cognitive therapy or cognitive training. On the pooled estimate, it did.
- Intervention: tDCS or related transcranial electrical stimulation paired with cognitive training.
- Comparator: Cognitive training or cognitive stimulation without the added electrical stimulation.
- Main readout: Global cognitive performance measured with scales such as the Montreal Cognitive Assessment (MoCA), Mini-Mental State Examination (MMSE), WAIS, ADAS-Cog, CVLT, or PASAT.
- Main result: A modest short-term improvement that did not prove durable across follow-up.
The Treatment Mix Was Broad, Not One Standard Protocol
The included studies were not testing a single clinic-ready recipe. Most used anodal stimulation, often targeting the dorsolateral prefrontal cortex (DLPFC), a frontal executive-control region, but the exact montage, dose, duration, training task, and patient group varied.
That variation is the main reason the result should be read carefully. The review found I2 = 55% for the global cognitive outcome, which means a meaningful share of the differences between trial results was not just random noise.
Typical stimulation sessions clustered around 20 minutes, with many protocols using 2.0 mA current and training several times per week. But the studies still differed in enough ways that the pooled estimate cannot tell a clinician exactly where to place electrodes or how many sessions to prescribe.
Stroke and PPA Looked More Promising Than MCI
The subgroup pattern was uneven. The largest cognitive effect appeared in primary progressive aphasia (PPA), a language-led neurodegenerative syndrome, with an SMD of 0.82.
Post-stroke cognitive impairment followed with an SMD of 0.65, though its confidence interval crossed zero. Mild cognitive impairment had an SMD of 0.15, and multiple sclerosis had an SMD of 0.07.
Those numbers suggest little to no clear cognitive advantage in the mild-cognitive-impairment and multiple-sclerosis subgroups in this dataset.
- PPA: The signal was largest, but it came from a small evidence base.
- Post-stroke impairment: Cognitive and daily-function outcomes looked more favorable than in several other conditions.
- Mild cognitive impairment: The pooled cognitive effect was small and did not reach the same practical threshold.
- Multiple sclerosis: The estimate was close to no effect, with wide uncertainty.
Subgroup comparisons did not prove that one diagnosis truly responds better than another. They do show why a one-size-fits-all tDCS headline would be misleading.
Daily Function Improved Mainly in Post-Stroke Studies
Cognitive test scores are not the same thing as everyday independence. The review also examined functional performance, including activities of daily living and independence scales.
The overall functional estimate was SMD 0.41, but its confidence interval ranged from -0.09 to 0.91, so the pooled functional result was not statistically secure.
The clearest functional signal came from post-stroke cognitive impairment. In that subgroup, the functional-performance estimate was SMD 0.97, with a 95% confidence interval from 0.34 to 1.59.
That is potentially meaningful, but it should be interpreted as condition-specific and still in need of stronger replication.
For Alzheimer’s disease, HIV-associated cognitive impairment, and PPA, functional evidence was smaller, thinner, or very uncertain. A treatment that changes a cognitive scale without reliably changing daily function may still be relevant, but it should not be oversold as life-changing rehabilitation.
Why the Evidence Is Still Too Uncertain for a Protocol
The strongest conclusion is not that tDCS fails. It is that the current evidence is not yet clean enough to define who should receive it, at what target, for how long, and with which cognitive task.
- Imprecision: Several confidence intervals crossed important effect-size thresholds.
- Heterogeneity: Studies varied by diagnosis, electrode montage, stimulation dose, training task, and outcome scale.
- Risk of bias: Some trials did not clearly report whether outcome assessors were blinded.
- Durability: Benefits were clearest immediately after treatment and weakened across follow-up.
For patients and clinicians, the practical takeaway is modest. tDCS plus cognitive training may be a reasonable adjunct in selected rehabilitation settings, especially where stimulation is tightly paired with the trained task.
The evidence does not support treating it as a stand-alone cognitive rescue treatment.
The next high-value trials would be narrower: one condition, one stimulation target, one training approach, and follow-up long enough to show whether gains persist. Until then, the evidence is encouraging but not settled.
Citation: DOI: 10.64898/2026.04.26.26351755. Soto-Fernandez Soto-Fernandez et al. Effects of transcranial direct current stimulation (tDCS) combined with cognitive therapy in individuals with cognitive impairment: a systematic review and meta-analysis. medRxiv . 2026. medRxiv. 2026.
Study Design: Systematic review and meta-analysis of randomized or controlled clinical trials.
Sample Size: 27 studies and 1,012 participants in the main quantitative evidence set.
Key Statistic: Global cognitive performance favored tDCS plus cognitive training, SMD 0.36 (95% CI: 0.15 to 0.56).
Caveat: This is a non-peer-reviewed preprint, and the review rated the evidence certainty as very low.