TL;DR: A 2026 narrative review in Journal of Central Nervous System Disease found that glucagon-like peptide-1 receptor agonists have promising stroke-prevention and animal-model evidence, but human data do not yet support routine use as an acute ischemic stroke neuroprotective treatment.
Key Findings
- Search through January 2026: The review covered preclinical stroke models, observational studies, randomized trials, and meta-analyses involving GLP-1 receptor agonists.
- 12 post-stroke animal studies: Table 1 summarized GLP-1 receptor agonist treatment after stroke onset across middle cerebral artery and carotid occlusion models.
- REWIND stroke reduction: Dulaglutide was linked to lower total stroke risk in REWIND, with a hazard ratio of 0.76 and a 95% CI of 0.62 to 0.94.
- SUSTAIN-6 nonfatal stroke finding: Subcutaneous semaglutide was linked to lower nonfatal stroke risk, with a hazard ratio of 0.61 and a 95% CI of 0.38 to 0.99.
- Acute AIS evidence remains insufficient: Small acute stroke trials mainly support feasibility and metabolic safety, not proven neuroprotection.
Source: Journal of Central Nervous System Disease (2026) | Samanidou et al.
GLP-1 receptor agonists such as semaglutide, liraglutide, dulaglutide, exenatide, and related drugs now sit at the intersection of diabetes, obesity, cardiovascular prevention, and brain health. Stroke is where the excitement needs the most discipline.
Samanidou and coauthors reviewed whether these drugs should be considered for acute ischemic stroke (AIS), secondary stroke prevention, or both. Their answer separates three evidence lanes that are often blurred together.
Animal Stroke Models Showed GLP-1 Neuroprotection Findings
The strongest mechanistic evidence came from cell and animal studies. In stroke models, GLP-1 receptor agonist exposure was repeatedly linked to lower infarct volume, improved neurological outcomes, and changes in biological pathways that matter after brain ischemia.
The review highlighted several proposed mechanisms:
- Less excitotoxic injury: GLP-1 signaling may reduce glutamate-related calcium stress in neurons.
- Less cell death: Animal models showed antiapoptotic patterns, including higher Bcl-2 and lower Bax or caspase-3 markers.
- Less inflammation and oxidative stress: Studies reported lower inflammatory markers and better redox status after treatment.
- Better vascular repair: Some models showed improved blood flow, blood-brain barrier integrity, angiogenesis, or neurogenesis markers.
Those findings are biologically plausible. They do not mean the same effect has been proven in people arriving at an emergency department with a blocked artery.
The animal studies varied by drug, dose, route, stroke model, and timing. Some used intracerebral or intracerebroventricular delivery, which bypasses the normal blood-brain barrier and is not how these medications are used clinically.
Stroke Prevention Evidence Came From Cardiometabolic Trials
The human prevention evidence mostly comes from cardiovascular outcome trials, where stroke was usually a secondary endpoint. These trials were designed around diabetes, obesity, kidney disease, or cardiovascular risk, not acute stroke neuroprotection.
Several results were still clinically relevant:
- Dulaglutide in REWIND: Total stroke risk was lower with dulaglutide, with a hazard ratio of 0.76.
- Semaglutide in SUSTAIN-6: Nonfatal stroke risk was lower with subcutaneous semaglutide, with a hazard ratio of 0.61.
- Meta-analysis estimate: One 2023-era meta-analysis of 11 CVOTs and 82,140 participants found a 16% relative reduction in stroke risk.
These data support GLP-1 receptor agonists as part of long-term risk management when a patient already has an established indication, such as type 2 diabetes, obesity, atherosclerotic cardiovascular disease, or high cardiometabolic risk.
They do not define the dose, timing, or patient group for treating an acute stroke as it is happening.
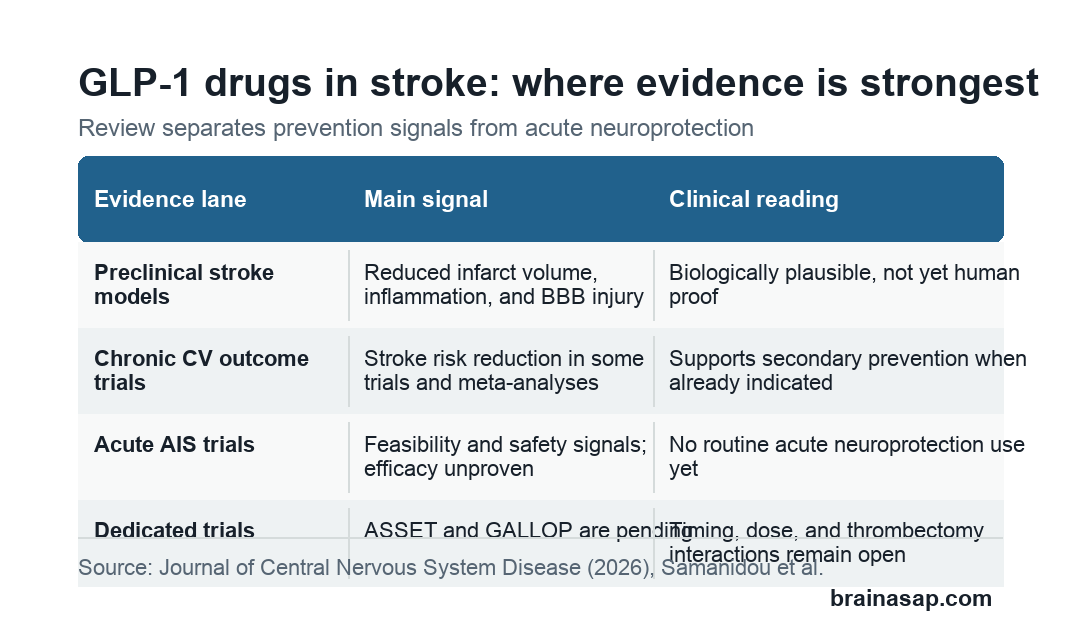
Acute Ischemic Stroke Trials Have Not Proven Neuroprotection
The acute-stroke evidence is much thinner. A small exenatide pilot study in 11 patients with acute stroke found treatment was tolerated for post-stroke hyperglycemia management and did not produce symptomatic hypoglycemia.
A prehospital exenatide trial enrolled only 19 patients before early termination, so it could not answer efficacy. The TEXAIS phase II trial tested exenatide within 9 hours and did not improve neurological impairment at 7 days versus placebo, although it reduced hyperglycemic events without hypoglycemia.
The LAMP trial was more encouraging but still specific. It studied liraglutide in 636 patients with acute minor ischemic stroke or high-risk transient ischemic attack and type 2 diabetes in China.
Liraglutide was linked to lower stroke recurrence, with a hazard ratio of 0.56, and better 90-day outcomes, with an odds ratio of 1.95. Those results do not establish class-wide acute neuroprotection for broader AIS pathways.
Timing, Dosing, and Thrombectomy Interactions Remain Open
The review’s main caution is translational. Human stroke varies by artery, clot burden, collateral flow, infarct core, time to treatment, diabetes status, frailty, and access to thrombolysis or mechanical thrombectomy.
Future trials need to answer practical questions:
- Timing window: Should treatment start before reperfusion, after reperfusion, or during early recovery?
- Agent selection: Are semaglutide, liraglutide, exenatide, and dulaglutide meaningfully different for brain exposure or vascular effects?
- Procedure safety: Do delayed gastric emptying, vomiting, aspiration risk, or sedation workflows matter during thrombectomy or acute imaging?
- Patient selection: Should trials focus on diabetes, obesity, kidney disease, large-vessel occlusion, minor stroke, or patients without diabetes?
ASSET and GALLOP are examples of stroke-dedicated trials that may help clarify feasibility, safety, and outcomes. The review argues that future trials should include imaging, biomarkers, exposure-response measures, and functional endpoints rather than relying only on broad cardiovascular outcomes.
GLP-1 Stroke Evidence Supports Prevention Before Acute Use
The clean clinical reading is conservative. GLP-1 receptor agonists can be considered for secondary prevention when patients have standard indications, but the review does not support adding them routinely as acute neuroprotective therapy for AIS.
That distinction protects patients from overreading animal data while preserving a useful prevention finding. A drug can reduce long-term stroke risk through weight, glucose, inflammation, blood pressure, endothelial function, or atherosclerotic pathways without directly rescuing threatened brain tissue during an acute infarct.
The next step is not a blanket recommendation. It is a set of stroke-specific trials that test the right drug, dose, timing, and population against the outcomes stroke clinicians actually need.
Citation: DOI: 10.1177/11795735261444425. Samanidou et al. GLP-1 Receptor Agonists in Acute Ischemic Stroke and Secondary Stroke Prevention: A Narrative Review of Preclinical and Clinical Evidence. Journal of Central Nervous System Disease. 2026;18:1-13.
Study Design: Narrative review of preclinical, observational, randomized, and meta-analytic evidence through January 2026.
Sample/Model: Evidence included animal stroke models, cardiovascular outcome trials, small acute AIS trials, and meta-analyses.
Key Statistic: One meta-analysis of 11 cardiovascular outcome trials and 82,140 participants found a 16% relative reduction in stroke risk with GLP-1 receptor agonists versus placebo.
Caveat: The review did not perform a formal risk-of-bias assessment or new quantitative meta-analysis.