TL;DR: A 2026 preprint in medRxiv surveyed people with multiple system atrophy and found that neurogenic orthostatic hypotension was often underdiagnosed, rarely fully controlled, and strongly tied to daily function and caregiver burden.
Key Findings
- 259 MSA respondents: The survey analyzed 259 people with self-reported multiple system atrophy, with mean age 64.38 years and 44% female participants.
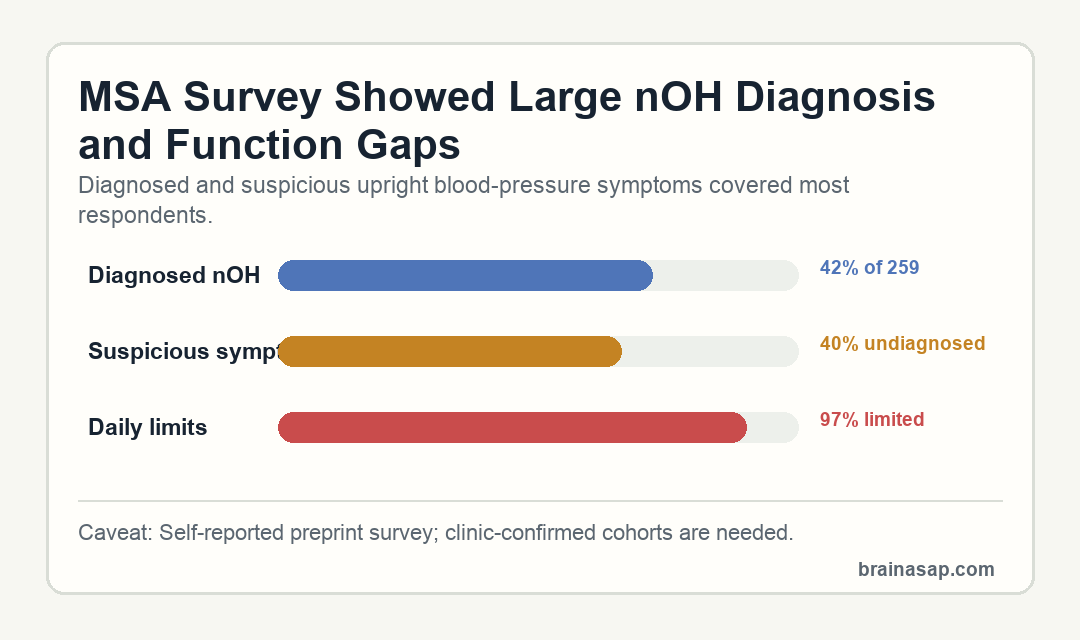
- 42% had diagnosed nOH: Neurogenic orthostatic hypotension was physician-diagnosed in 42% of respondents.
- 40% looked suspicious but undiagnosed: Another 40% reported upright symptoms highly suspicious for nOH without a diagnosis.
- Standing BP was often missed: 21% said their blood pressure had never been measured while standing during a clinical visit.
- Daily burden stayed high: Despite anti-hypotensive medication use, 97% reported limitations in bathing, cooking, or rising from a chair or bed, and 76% needed caregiver support for refractory nOH symptoms.
Source: medRxiv (2026) | Kmiecik et al.
Neurogenic orthostatic hypotension (nOH) is a drop in blood pressure on standing caused by autonomic nervous system failure. In multiple system atrophy, or MSA, it can cause dizziness, fatigue, fainting, falls, and cognitive difficulty when upright.
This study did not test a new drug. It asked people with MSA how nOH affected daily life: whether it was diagnosed, whether clinicians checked standing blood pressure, and whether treatment actually controlled symptoms.
MSA Survey Found Diagnosed and Undiagnosed nOH Burden
The cross-sectional online survey included 259 respondents with self-reported MSA. Mean age was 64.38 years, and 44% of respondents were female.
Within that group, 42% reported a diagnosis of nOH. Another 40% had symptoms highly suspicious for nOH but no diagnosis, suggesting that many patients may live with recognizable autonomic symptoms before formal recognition.
- Diagnosed nOH: 108 of 259 respondents met the highest-certainty MSA-with-nOH grouping.
- Suspicious symptoms: 103 respondents had upright symptoms consistent with nOH but no diagnosis.
- No nOH grouping: A smaller group did not fit the diagnosed or suspicious-symptom categories.
The clinical gap was also concrete. 21% of respondents said their blood pressure had never been measured in the standing position during a clinical visit.
Posture-dependent nOH requires posture-specific measurement. A seated or lying blood-pressure reading can miss the drop that appears when a patient stands, walks, showers, or gets out of bed.
Standing Symptoms Interfered With Basic Daily Activities
Among people with diagnosed nOH, symptoms were common while standing, rising from a chair, or walking. Dizziness or lightheadedness was one of the most common complaints, and many respondents also described fatigue, weakness, or cognitive/mood effects.
The functional numbers were striking. Despite anti-hypotensive medication use, 97% reported limitations in bathing, cooking, or getting up from a chair or bed, and 76% reported caregiver support for refractory nOH symptoms.
- Bathing and standing: Upright symptoms can make showering or personal care risky.
- Cooking and household tasks: Standing long enough to prepare food can become difficult.
- Chair or bed transfers: Rising from a seated or lying position can trigger blood-pressure drops.
Those activities describe loss of independence in a neurodegenerative disorder that already carries motor, autonomic, and caregiver strain.
The survey also showed a long path to recognition for many patients. Nearly half of diagnosed MSA-with-nOH respondents reported waiting at least one year after first noticing nOH symptoms before receiving a diagnosis.
Each Additional nOH Symptom Raised Medication Odds
Medication use tracked symptom burden, but it did not solve the problem for most respondents. Logistic regression showed that each additional nOH symptom increased the odds of taking blood-pressure medication by 18%.
Researchers also found that six nOH symptoms was the optimal cut point for identifying medication use by the Youden index, but symptom count alone did not cleanly classify who was using blood-pressure medication.
- Medication signal: More symptoms were associated with higher odds of pharmacotherapy.
- Residual burden: Many treated respondents remained limited by symptoms.
- Background MSA effects: Motor and other autonomic features also contributed to daily function.
The survey emphasized burden as well as diagnosis. nOH treatment may reduce blood-pressure symptoms for some patients, but the data suggest many people remain far from symptom control.
Non-drug approaches were common as well, with the study reporting high use of measures such as fluid, salt, compression, or positional strategies. Persistent symptoms despite those strategies make the remaining functional burden more clinically relevant.
Home Standing Blood Pressure May Be a Practical Screening Target
The study’s immediate implication is basic care quality: standing blood pressure should be checked when MSA patients report upright symptoms. The preprint also notes that many respondents would be willing to measure blood pressure at home to screen for nOH.
Because the survey was anonymous and self-reported, the results should not be treated as a clinic-confirmed prevalence estimate. Even with that limit, the 40% suspicious-but-undiagnosed group points to a symptom burden that patients can describe clearly.
- Strong point: The survey directly captured patient-reported daily limitations and caregiver needs.
- Main limit: Diagnosis, symptoms, and blood-pressure history were self-reported rather than clinically verified.
- Clinical question: Better screening and objective endpoints are needed to measure nOH burden in trials and care.
For MSA care, the clinical workflow is straightforward: if upright symptoms are present, standing blood pressure and treatment response should be made visible, not assumed.
That message is especially relevant for trials. If nOH symptoms fluctuate with posture, meals, time of day, and background MSA severity, future studies need objective endpoints that can separate blood-pressure physiology from broader disease disability.
Citation: DOI: 10.64898/2026.04.20.26351214. Kmiecik et al. The burden of neurogenic orthostatic hypotension in patients with multiple system atrophy – a real-world study. medRxiv. 2026.
Study Design: Cross-sectional anonymous online survey of people with self-reported multiple system atrophy.
Sample Size: 259 respondents with MSA; 108 had diagnosed nOH and 103 had suspicious upright symptoms without diagnosis.
Key Statistic: 97% of treated patients reported daily functional limitations, and each additional nOH symptom increased medication odds by 18%.
Caveat: This is a preprint survey with self-reported diagnoses and symptoms, not a clinic-confirmed cohort.