TL;DR: A 2026 preprint on medRxiv found that older adults with mild-cognitive-impairment-level scores showed different resting facial action patterns than healthy controls, especially upper lip raiser, lip tightener, and lip suck measures.
Key Findings
- MCI-level comparison: The study included 45 older adults and compared 31 participants in the MCI-level group with 14 healthy controls.
- MoCA-defined groups: Participants were classified using Montreal Cognitive Assessment-Japanese (MoCA-J) scores, with group means of 23.7 versus 27.1.
- 35 facial measures: Researchers analyzed intensity for 17 facial Action Units and presence or absence for 18 Action Units during rest.
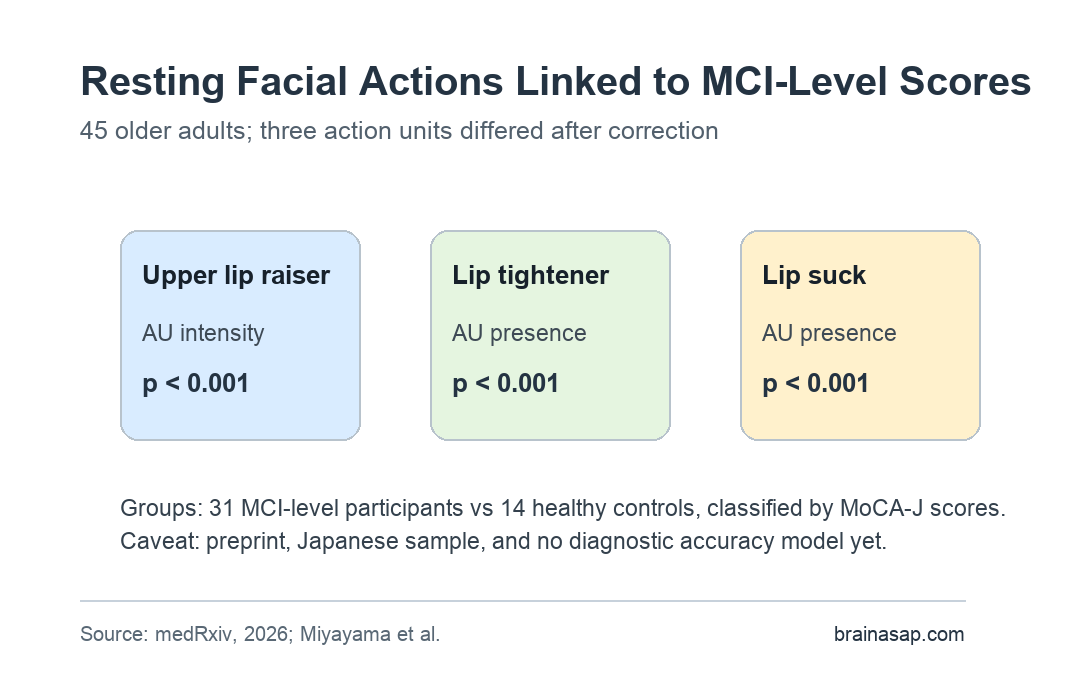
- Upper lip raiser: AU intensity for upper lip raiser differed between groups at p < 0.001 after multiple-comparison correction.
- 2 presence findings: Lip tightener and lip suck presence also differed between groups at p < 0.001 after correction.
Source: medRxiv (2026) | Miyayama et al.
Mild cognitive impairment (MCI) describes measurable cognitive decline that is greater than expected with normal aging but does not meet criteria for dementia. Detecting MCI earlier is difficult because many screening tools require appointments, trained staff, or formal cognitive testing.
The research team tested a different marker: facial expression at rest. The study asked whether video-based facial Action Units could distinguish older adults with MCI-level cognitive scores from healthy controls.
31 MCI-Level Participants Were Compared With 14 Healthy Controls
The sample included 45 Japanese older adults. The MCI-level group had 31 participants, while the healthy-control group had 14 participants.
Groups were assigned using the Montreal Cognitive Assessment-Japanese (MoCA-J), a cognitive screening test adapted for Japanese-language assessment. Mean MoCA-J scores were 23.7 in the MCI-level group and 27.1 in controls.
- Age balance: Mean age was 74.3 years in the MCI-level group and 73.9 years in controls.
- Depression screen: Geriatric Depression Scale scores did not differ between groups, with p = 0.74.
- Education split: The study recorded whether participants had at least 13 years of education, because education can affect cognitive screening performance.
This was not a dementia-diagnosis study. The paper used “MCI level” because grouping was based on cognitive-screening scores rather than a full clinical dementia-workup pathway.
35 Resting Facial Action Measures Were Extracted From Video
The facial-expression analysis used Action Units (AUs), a coding system that describes visible movements such as lip tightening, lip sucking, or raising part of the upper lip. Researchers extracted these measures from resting-state facial video.
Two statistical models were used. A multilevel zero-inflated beta regression tested 17 AU intensity measures, while a multilevel logistic regression tested the presence or absence of 18 AUs.
- Intensity model: This analysis asked whether the strength of a facial action differed between groups.
- Presence model: This analysis asked whether an action appeared at all during the resting recording.
- Correction step: The significant findings reported in the abstract remained significant after multiple-comparison correction.
The method is relevant because resting facial expression could, in theory, be captured in ordinary settings. The preprint does not yet show that such a tool is ready for clinics or home screening.
Upper Lip Raiser Intensity Differed Between MCI-Level and Control Groups
The intensity analysis found one corrected group difference. The upper lip raiser Action Unit differed between MCI-level participants and healthy controls at p < 0.001.
That result means the measured intensity of that facial movement was statistically associated with group status in this sample. It is not evidence that an observer could diagnose MCI by watching one person’s mouth at rest.
- Measure type: The result came from computer-extracted AU intensity, not a clinician’s visual impression.
- Context: The study focused on resting expression, not emotion recognition, conversation, or posed facial movement.
- Interpretation: The finding is a candidate marker that needs replication and diagnostic testing.
For Alzheimer’s disease research, the distinction is useful. A subtle facial marker could become part of unobtrusive screening, but only if future work shows that it holds across settings, cultures, cameras, and clinical groups.
Lip Tightener and Lip Suck Presence Also Differed at p < 0.001
The presence-or-absence model identified two additional corrected findings. Lip tightener and lip suck both differed between groups at p < 0.001.
These were binary-style findings: whether the facial action appeared during the resting recording. Together with the intensity result, the findings suggest that resting facial behavior may contain measurable cognitive-status information.
- Not a stand-alone test: The study did not report a deployed screening threshold, sensitivity, specificity, or real-world false-positive rate.
- Not diagnosis: The group label came from MoCA-J scores, not from a full biomarker-confirmed Alzheimer’s disease diagnosis.
- Not culture-free: All participants were Japanese, so cross-cultural replication is needed.
The most practical conclusion is that facial-expression analysis may be worth adding to broader MCI screening research. It should not replace cognitive evaluation, clinical history, or biomarker work.
Japanese Sample and Biometric Recruitment Limit Generalization
Several limitations are central to this topic. The sample was small, all participants were Japanese, and people uncomfortable with facial biometric data may have opted out before enrollment.
Trust is central because a facial-video screening tool depends on voluntary biometric data. People who avoid biometric data collection may be underrepresented in the dataset used to build or test the tool.
- Sample size: The study had 31 MCI-level participants and 14 controls, so larger validation samples are needed.
- Population scope: Findings need replication across cultures, languages, clinical settings, and camera environments.
- Clinical endpoint: Future studies should test whether facial markers predict conversion, biomarker status, or clinician-diagnosed MCI.
The preprint’s strongest contribution is its narrow result: resting facial Action Units showed corrected group differences in a small older-adult sample. The next step is to test whether those markers improve screening accuracy when added to existing cognitive and clinical measures.
Citation: DOI: 10.64898/2026.04.10.26350581. Miyayama et al. Characteristic resting state facial expressions in older adults with mild cognitive impairment level. medRxiv. 2026.
Study Design: Cross-sectional preprint study of resting facial Action Units in older adults classified by MoCA-J cognitive screening scores.
Sample Size: 31 MCI-level participants and 14 healthy controls.
Key Statistic: Upper lip raiser intensity, lip tightener presence, and lip suck presence each differed between groups at p < 0.001 after correction.
Caveat: The source is a preprint, the sample was small and Japanese, and the study did not validate a clinical screening threshold.