TL;DR: A 2026 study in Behavior Genetics found that combining major depressive disorder and alcohol use disorder polygenic scores improved prediction of their comorbidity in 7,965 Add Health participants, but added little for either condition alone.
Key Findings
- Add Health dataset anchored the analysis: The study used 7,965 European, African, and Admixed American ancestry participants from the National Longitudinal Study of Adolescent to Adult Health.
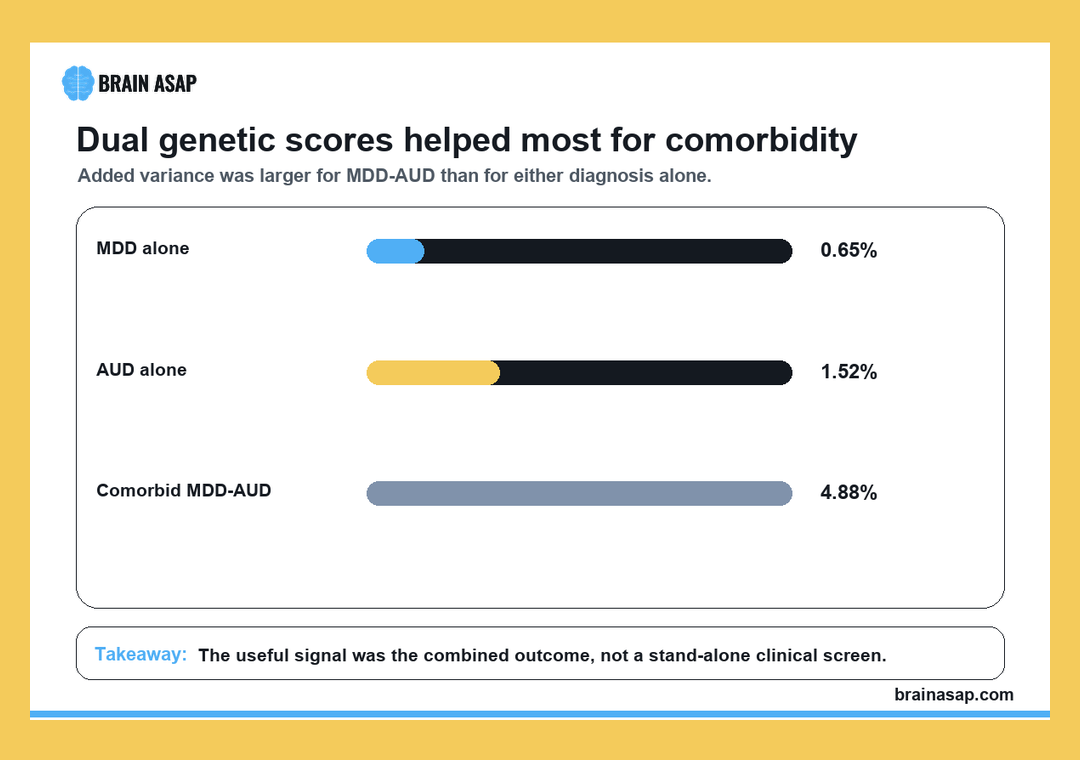
- Comorbidity prediction improved most: A model with both major depressive disorder (MDD) and alcohol use disorder (AUD) polygenic scores explained 4.88% additional variance for comorbid MDD-AUD.
- AUD genetic score was stronger for comorbidity: In the comorbid model, the AUD polygenic score had OR = 1.77, compared with OR = 1.26 for the MDD polygenic score.
- Single-disorder gains were smaller: The MDD score added 0.65% variance for MDD prediction, while the AUD score added 1.52% variance for AUD prediction.
- Adding both scores did not help every outcome: Including both scores improved comorbid MDD-AUD prediction but did not significantly improve models for MDD alone or AUD alone.
Source: Behavior Genetics (2026) | Wells et al.
MDD and AUD Polygenic Scores Were Tested Together
Polygenic scores (PGS) estimate inherited liability by combining many genetic variants, each with a small association from genome-wide studies. They are not diagnostic tests, and they do not determine whether a person will develop a disorder.
This study asked a narrower prediction question. If major depressive disorder and alcohol use disorder share some genetic liability, would using both PGS improve prediction of comorbid MDD-AUD more than using a single score?
The sample came from the National Longitudinal Study of Adolescent to Adult Health, often called Add Health. The analysis included 7,965 participants from European, African, and Admixed American ancestry groups.
Researchers built cross-ancestry scores with PRS-CSx, a method designed to combine genome-wide association information across ancestry groups. They then tested prediction for 3 outcomes:
- MDD: lifetime major depressive disorder.
- AUD: alcohol use disorder, based on DSM-IV alcohol abuse or dependence criteria.
- Comorbid MDD-AUD: participants who met criteria for both lifetime MDD and AUD.
The main comparison was not whether genetics predicts everything. It was whether a genetically correlated second score adds information beyond demographics and the primary disorder score.
Both Scores Improved Comorbid MDD-AUD Prediction
The clearest result was for comorbidity. The best-fitting whole-sample model for comorbid MDD-AUD included both the MDD PGS and the AUD PGS.
In that model, the MDD polygenic score had OR = 1.26 (95% CI 1.16 to 1.35), while the AUD polygenic score had OR = 1.77 (95% CI 1.66 to 1.87). Higher scores were associated with higher odds of comorbid MDD-AUD.
The combined score model explained an additional 4.88% of variance compared with a model that only included sociodemographic covariates.
The result supports the study’s central idea. Comorbidity may be better captured when genetic liability for both contributing conditions is modeled together.
Single-Disorder Models Gained Less From Extra Scores
The results for MDD alone and AUD alone were more modest. The best-fitting MDD model used the MDD PGS, with OR = 1.25 (95% CI 1.17 to 1.33) and an additional 0.65% of variance, while the best-fitting AUD model used the AUD PGS, with OR = 1.37 (95% CI 1.32 to 1.43) and an additional 1.52% of variance.
Adding the genetically correlated second score did not significantly improve prediction for MDD alone or AUD alone. The paper therefore separates 2 claims:
- Comorbidity claim: using both PGS improved prediction when the outcome was having both MDD and AUD.
- Single-disorder claim: each condition was predicted best by its own disorder-specific score.
- Clinical claim: the added variance remained limited, so these scores are research tools rather than stand-alone clinical screeners.
This distinction is important for interpreting psychiatric genetics. A statistically significant PGS can still explain a small share of individual outcome variation.
Cross-Ancestry Scoring Addressed a Common Genetics Limitation
Psychiatric genetic studies have often performed best in people whose ancestry resembles the discovery genome-wide association sample. That creates equity and validity problems when findings are applied to broader populations.
Wells et al. used PRS-CSx, which combines ancestry-specific information to create cross-ancestry polygenic scores.
The Add Health sample included European, African, and Admixed American ancestry participants, making the design more informative than a single-ancestry analysis.
Even so, cross-ancestry scoring does not eliminate all problems. Prediction can still differ by ancestry because discovery datasets, linkage disequilibrium patterns, social exposures, and phenotype definitions vary.
The authors also had to align psychiatric definitions across datasets. AUD was based on DSM-IV alcohol abuse or dependence criteria, while the genetic discovery work and modern clinical language may use related but not identical definitions.
- Genetic liability: PGS captures inherited statistical risk, not destiny.
- Environmental context: alcohol availability, stress, trauma, treatment access, and social support are not reduced to DNA.
- Comorbidity complexity: MDD and AUD can co-occur through shared biology, causal pathways, or shared life exposures.
Comorbid Depression and AUD Need More Than Single-Risk Models
The practical takeaway is that comorbid psychiatric outcomes may need models built for comorbidity, not just separate models stitched together afterward.
For research, that means genetically correlated traits can add information when the outcome itself combines 2 conditions. For clinical care, the current numbers are too small for deterministic individual prediction.
A PGS result cannot say whether a person will develop depression, alcohol use disorder, or both. It can help researchers estimate liability patterns in large groups and test how shared genetic risk contributes to overlapping disorders.
The supported claim is specific: in Add Health, combined MDD and AUD polygenic scores improved prediction of comorbid MDD-AUD more than they improved prediction of either diagnosis alone.
Citation: DOI: 10.1007/s10519-026-10263-3. Wells et al. The Contributions of Multiple Polygenic Scores in Predicting Liability for Major Depressive Disorder and Its Comorbidity with Alcohol Use Disorder. Behavior Genetics. 2026.
Study Design: Genetic prediction analysis using cross-ancestry polygenic scores in Add Health participants.
Sample Size: 7,965 European, African, or Admixed American ancestry participants.
Key Statistic: The dual-score comorbidity model added 4.88% variance; MDD PGS OR = 1.26 and AUD PGS OR = 1.77 for comorbid MDD-AUD.
Caveat: Polygenic scores explain limited variance and are not diagnostic or deterministic clinical tests.