TL;DR: A 2026 systematic review and Bayesian meta-analysis in Journal of Medical Internet Research found that artificial intelligence models trained only on overnight pulse-oximetry oxygen-saturation data detected obstructive sleep apnea with 91.1% sensitivity and 88.4% specificity across 25 studies.
Key Findings
- 25 studies and 23,171 participants were included: The review pooled adult studies that compared AI models using oxygen saturation (SpO2) recordings against apnea-hypopnea index (AHI)-defined sleep apnea.
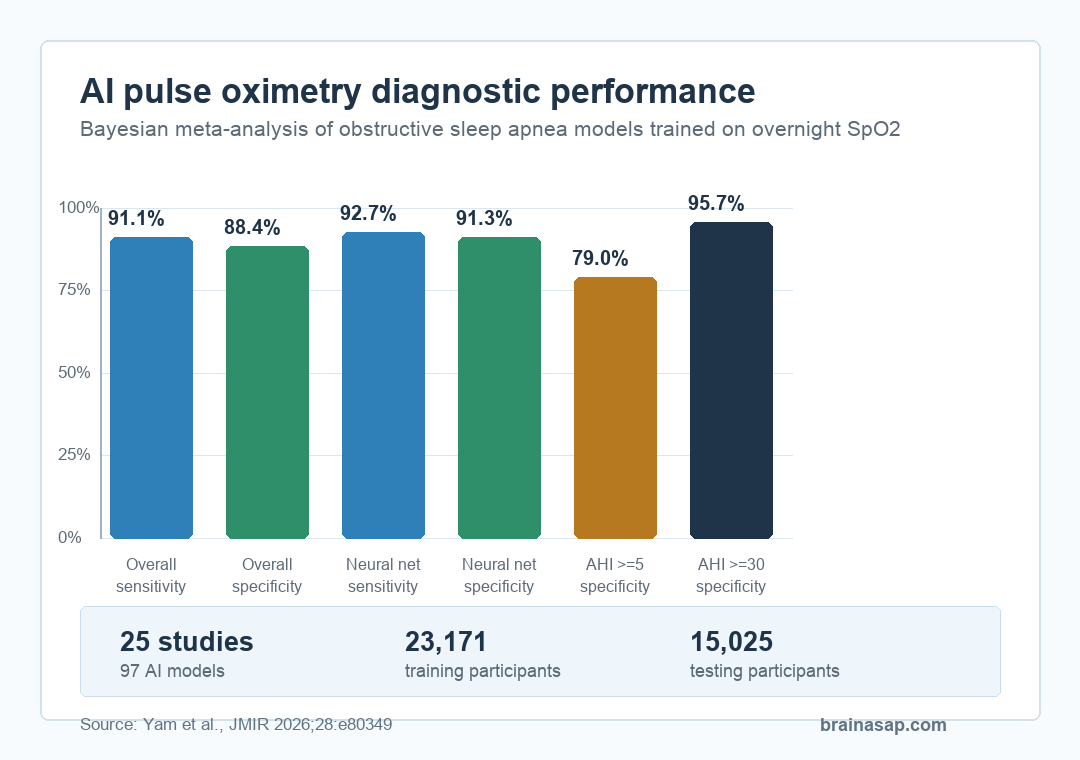
- Overall diagnostic performance was high: AI-oximetry models reached 91.1% sensitivity and 88.4% specificity, with a negative likelihood ratio of 0.10.
- Neural-network classifiers performed best: Neural networks reached 92.7% sensitivity and 91.3% specificity in subgroup analysis.
- Severity thresholds shifted the tradeoff: Sensitivity was highest at AHI ≥5, while specificity rose to 95.7% at AHI ≥30.
- Real-world validation is still the main limit: Most studies used retrospective or sleep-clinic datasets, so primary-care and low-prevalence settings still need prospective testing.
Obstructive sleep apnea is often missed because the standard test, overnight polysomnography, is expensive, labor-intensive, and hard to scale. Pulse oximetry is much simpler: it tracks blood oxygen saturation through a small sensor, usually on a finger.
The question in this review was whether AI analysis of overnight oxygen-saturation patterns can turn that simpler signal into a reliable diagnostic test. The pooled estimates showed strong diagnostic accuracy, but that is not the same as saying a finger sensor can fully replace a sleep lab.
AI Oximetry Detected Sleep Apnea With High Sensitivity
The meta-analysis included 25 cross-sectional diagnostic-accuracy studies and 97 AI models. Together, the studies covered 23,171 participants used to train models and 15,025 participants used for testing.
All models used oxygen-saturation recordings and were judged against the apnea-hypopnea index, or AHI, the standard count of breathing pauses or shallow-breathing events per hour of sleep. Across models and thresholds, AI oximetry reached:
- 91.1% sensitivity: about 91 of 100 people with obstructive sleep apnea would be flagged by the model.
- 88.4% specificity: about 88 of 100 people without obstructive sleep apnea would be correctly classified as not having it.
- Negative likelihood ratio of 0.10: a negative result substantially lowered the probability of disease in the studied populations.
Those numbers are stronger than a simple oxygen-desaturation index alone and compare favorably with some home sleep apnea test approaches. Overnight oxygen data are also cheap and easy to collect compared with full polysomnography.
Neural Networks Had the Strongest Specificity
Different model families were not identical. Neural-network classifiers had the best combined performance, with 92.7% sensitivity and 91.3% specificity. Support-vector-machine models had similar sensitivity but lower specificity.
The review also separated how models extracted features from the oxygen signal. Models using deep learning feature extraction had higher sensitivity than models relying on manually selected expert features, by 3.7 percentage points.
That distinction is important. Oxygen saturation is not just one low-number event. The useful information may sit in the shape, timing, frequency, and clustering of desaturations across the night. AI models can learn those patterns from the raw signal rather than depending only on a small set of hand-built summary indices.
Sleep-Apnea Severity Changed the False-Positive Tradeoff
The model performance shifted depending on the AHI threshold used to define a positive case. At AHI ≥5, a threshold that captures mild obstructive sleep apnea, sensitivity was highest at 93.4%, but specificity was lower at 79.0%.
At AHI ≥30, a threshold for severe obstructive sleep apnea, specificity rose to 95.7%, while sensitivity was 88.1%. In plain terms, AI oximetry looked better at confidently identifying more severe disease, while lower thresholds caught more possible cases at the cost of more false positives.
- For screening: high sensitivity at lower AHI thresholds could help rule out low-risk patients or decide who needs formal testing.
- For case identification: high specificity at severe thresholds could help identify patients likely to need faster diagnostic follow-up.
- For final diagnosis: the model still cannot stage sleep, detect arousals, or distinguish obstructive from central apnea the way fuller sleep testing can.
The Evidence Was Strongest for Research Settings
The review used QUADAS-2 to assess diagnostic-study bias and GRADE to judge evidence certainty. The pooled evidence was rated high overall, and sensitivity analyses suggested that publication bias would not substantially change the main result.
Even so, the authors were careful about clinical readiness. Many included studies were retrospective, used sleep-clinic or hospital populations, and tested models in groups with high pretest probability of obstructive sleep apnea. Performance can look different when a test moves into primary care, where many more people do not have the disease.
Pulse oximetry also has physical limits. Motion artifact, probe displacement, temperature, anemia, hemoglobin disorders, nail varnish, and skin-pigmentation effects can all affect oxygen-saturation readings. A model trained on clean research data may not behave the same way on noisy home recordings.
AI Oximetry Could Triage Sleep-Apnea Testing
The practical result is not that AI oximetry should replace sleep laboratories. It is that single-channel overnight oxygen data may be more diagnostically useful than older oximetry summaries suggested.
A scalable workflow could use AI oximetry as a first-pass test: patients with strongly negative results might avoid unnecessary lab testing, while patients with high-risk patterns could move faster to home sleep apnea testing, polysomnography, or treatment evaluation. That would be especially useful in primary care, inpatient settings, and regions where sleep-lab access is limited.
The next evidence step is prospective external validation. The models need to be tested in diverse, lower-prevalence, real-world populations using the actual devices and workflows that clinics would use. Until then, the best reading is specific: AI models trained on overnight SpO2 data showed strong pooled diagnostic accuracy in published studies, but implementation still needs real-world proof.
Citation: DOI: 10.2196/80349. Yam et al. Artificial Intelligence Diagnosis of Obstructive Sleep Apnea Using Overnight Pulse Oximetry: A Systematic Review and Bayesian Meta-Analysis. Journal of Medical Internet Research. 2026;28:e80349.
Study Design: Systematic review and Bayesian diagnostic-test-accuracy meta-analysis registered with PROSPERO.
Sample Size: 25 studies, 97 AI models, 23,171 participants in training datasets, and 15,025 participants in testing datasets.
Key Statistic: Overall pooled sensitivity was 91.1% and specificity was 88.4%; neural-network classifiers reached 92.7% sensitivity and 91.3% specificity.
Caveat: Most included studies were retrospective or sleep-clinic based, so prospective validation in primary-care and low-prevalence settings is still needed.