TL;DR: A 2026 systematic review in European Archives of Psychiatry and Clinical Neuroscience argues that catatonia, a syndrome of freezing, mutism, and abnormal movement, may involve underweighted limbic-system circuitry linking emotional regulation with motor shutdown.
Key Findings
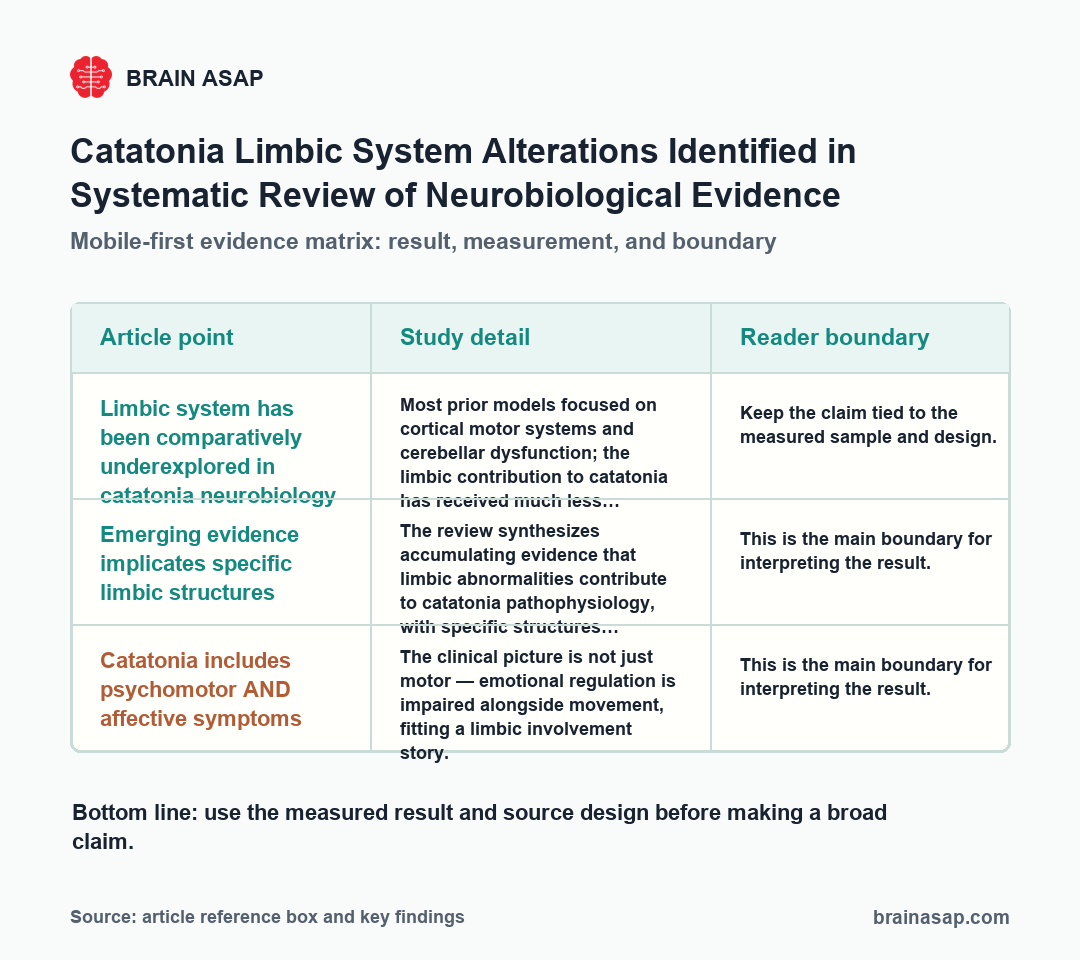
- Limbic system has been comparatively underexplored in catatonia neurobiology: Most prior models focused on cortical motor systems and cerebellar dysfunction; the limbic contribution to catatonia has received much less systematic attention.
- Emerging evidence implicates specific limbic structures: The review synthesizes accumulating evidence that limbic abnormalities contribute to catatonia pathophysiology, with specific structures emerging as candidate contributors.
- Catatonia includes psychomotor AND affective symptoms: The clinical picture is not just motor — emotional regulation is impaired alongside movement, fitting a limbic involvement story.
- PRISMA-guided systematic review of MEDLINE, Web of Science, PsycINFO: The methodology covers the available neurobiological evidence rather than relying on selective citation.
- The “frozen emotions, frozen bodies” frame is mechanistically substantive: The paper’s title is more than rhetorical — it captures a real conceptual shift toward viewing catatonia as a coupled disorder of emotional regulation and motor expression rather than a pure motor phenomenon.
- Treatment implications follow if limbic involvement is real: Standard catatonia treatment (benzodiazepines, ECT) works through mechanisms compatible with limbic modulation. Understanding the limbic substrate could refine when and how these treatments work best.
Source: European Archives of Psychiatry and Clinical Neuroscience (2026) | Marcolini, Beghelli, Tartarini, Di Giacomo, Tempia Valenta, Mastellari, De Ronchi, Atti
Catatonia can involve hours of immobility, mutism, refusal to eat, repeated words or movements, and waxy flexibility, where a person resists movement and then holds the imposed posture.
Most recent neuroscience work has framed catatonia as a problem of cortical motor systems and cerebellar regulation. The review team argues that this framing misses the limbic component.
Catatonia Includes Motor and Affective Symptoms
Catatonia presents with a constellation of motor and behavioral features that can include:
- Stupor — reduced responsiveness despite intact consciousness.
- Mutism — absent or severely reduced verbal output.
- Posturing — holding awkward, often physically uncomfortable positions for extended periods.
- Waxy flexibility — resistance to passive movement followed by maintaining the imposed position.
- Negativism — refusing instructions or doing the opposite.
- Echolalia and echopraxia — repeating others’ words or movements.
- Excited catatonia — the alternative form, with extreme agitation and purposeless movement.
Catatonia occurs across psychiatric and medical conditions — in mood disorders, schizophrenia, autoimmune encephalitis, metabolic disturbances, and more.
It’s a syndrome, not a single disease, which is part of why understanding its neurobiology has been so hard. Multiple causal pathways probably converge on a common circuit dysfunction that produces the catatonic phenotype.
Why the Limbic System Was Missing From Most Accounts
Catatonia neuroscience has historically focused on:
- Cortical motor systems — the supplementary motor area, premotor cortex, and primary motor cortex, which control voluntary movement.
- Cerebellar contributions — given the cerebellum’s role in movement coordination and increasingly in cognition.
- Frontal-subcortical loops — circuits connecting prefrontal cortex with basal ganglia and thalamus that support goal-directed behavior.
- GABA neurotransmission — particularly because benzodiazepines (which enhance GABA signaling) often produce dramatic catatonia improvement.
What’s been missing from this picture is systematic attention to the limbic system — the brain’s emotional regulation network including amygdala, hippocampus, anterior cingulate, insula, hypothalamus, and connected structures.
The review argues this gap is important because catatonia is not just a motor phenomenon — it includes affective symptoms that limbic involvement would naturally explain.
How “Frozen Emotions, Frozen Bodies” Captures a Real Conceptual Shift
The Marcolini paper’s title isn’t just literary. It captures a substantive reframing of catatonia:
- Old model: Catatonia is a motor system disorder. Patients can’t move properly because cortical and cerebellar motor control has failed. Affective symptoms are secondary.
- Emerging model: Catatonia is a coupled disorder of emotional regulation and motor expression. The freezing reflects a system-level shutdown that affects both how patients feel and how they move — because the same neural systems coordinate both.
The integrative framing fits clinical observation: catatonic patients describe, when they recover, intense fear, helplessness, or dissociation during episodes.
They are not just unable to move; they are often unable to engage emotionally with their environment. Treating motor shutdown and affective shutdown as separate problems misses the coupled nature of the dysfunction.
Limbic Involvement Could Affect Treatment Mechanisms
The standard treatments for catatonia are benzodiazepines, especially lorazepam, and electroconvulsive therapy (ECT). Both can work dramatically, but the mechanisms underlying their effectiveness have not been fully explained, and a limbic involvement model offers possible insights:
- Benzodiazepines enhance GABA transmission throughout the brain, including in limbic structures. Their dramatic effect on catatonia could partly reflect limbic-system modulation rather than only cortical motor circuit effects.
- ECT affects limbic structures particularly strongly, producing widespread changes in hippocampal and amygdala function. The treatment’s effectiveness for catatonia could partly reflect direct limbic effects.
- Refractory catatonia — cases that don’t respond to standard treatment — may involve different limbic involvement patterns than responsive cases. Subtyping by limbic profile could potentially guide treatment selection.
- NMDA-antagonist approaches (memantine, amantadine) have shown some efficacy in catatonia and act on systems involving limbic structures, fitting the limbic model.
What a Systematic Review Can and Cannot Establish
Systematic reviews are good at synthesizing what’s been published. They have limits:
- Existing literature was the input. If the field has historically underweighted limbic studies, the review can synthesize what exists but can’t generate new evidence.
- Heterogeneous methodology across included studies makes meta-analysis difficult; qualitative synthesis is what’s typically possible.
- Catatonia is rare and heterogeneous. Most studies use small samples; replicable findings across studies are harder to establish.
- The argument is “limbic system deserves more attention,” not “limbic system is the cause.” The review identifies a research gap and the converging evidence pointing toward it — not a definitive mechanistic account.
Why This Reshapes Where Catatonia Research Should Go Next
The Marcolini synthesis points to specific research priorities:
- Limbic-focused neuroimaging in catatonic patients — structural and functional imaging with explicit hypotheses about amygdala, anterior cingulate, hippocampus, and insula involvement.
- Limbic-cortical coupling analysis — rather than studying motor circuits in isolation, examining how limbic and motor systems interact during catatonia and recovery.
- Affective phenotyping in catatonia studies — capturing the emotional component systematically alongside motor symptoms.
- Treatment-response stratification by limbic involvement — testing whether limbic profile predicts response to benzodiazepines, ECT, NMDA antagonists, or other interventions.
- Animal models that capture both motor and affective components — current models often emphasize motor freezing without parallel emotional measures.
Boundary on this reframing:
The review makes a measured argument: limbic involvement deserves systematic attention in catatonia neurobiology, and current evidence already supports specific limbic structures as candidate contributors. What it doesn’t claim:
- Cortical and cerebellar accounts: these models are incomplete, not wrong.
- Heterogeneity: all catatonia does not have to involve the same limbic dysfunction.
- Treatment readiness: the implication is a research direction, not a treatment recommendation.
- Case coverage: some cases with clear cortical lesions or cerebellar involvement may not fit a limbic-centered framework.
Clinical recognition:
One downstream effect of the limbic reframing is on diagnostic recognition. If catatonia involves frozen emotional regulation alongside frozen movement, clinicians paying attention to affective signs — flat or absent emotional engagement, dissociation, fearful immobility — may catch catatonia earlier and more often than purely motor-based recognition.
Catatonia is significantly underdiagnosed in psychiatric and medical inpatient settings.
Part of the underdiagnosis is that purely motor presentations dominate the textbook picture, while subtler presentations — affective freezing, emotional withdrawal, partial responsiveness — can be missed.
The limbic framework may help clinicians recognize the syndrome across its full presentation rather than only in its most florid forms.
Citation: DOI: 10.1007/s00406-026-02244-8. Marcolini F, Beghelli V, Tartarini D, Di Giacomo V, Tempia Valenta S, Mastellari T, De Ronchi D, Atti AR. Frozen emotions, frozen bodies: a systematic review of limbic system alterations in catatonia. European Archives of Psychiatry and Clinical Neuroscience. 2026.
Study Design: PRISMA-guided systematic review across MEDLINE, Web of Science, and PsycINFO synthesizing neurobiological evidence on limbic system alterations in catatonia.
Source Coverage: Studies addressing limbic system involvement in catatonia — see full publication for inclusion criteria and study count.
Key Statistic: Limbic system involvement in catatonia has been comparatively underexplored relative to cortical and cerebellar models; emerging evidence supports specific limbic structures as contributors to the catatonic syndrome, integrating affective and motor symptoms within a coupled framework.
Caveat: Systematic reviews synthesize existing evidence rather than generating new data; catatonia literature is heterogeneous and often based on small samples; the argument is for greater research attention to limbic involvement, not for a fully validated limbic-centered model of catatonia pathophysiology.
Sample Size: Published catatonia neurobiology studies identified through MEDLINE, Web of Science, and PsycINFO.