TL;DR: A 2025 randomized trial in Scandinavian Journal of Primary Health Care found that a self-help book based on cognitive behavioral therapy for insomnia (CBT-I), a structured non-drug insomnia treatment, reduced daily hypnotic sleep-medication use and anxiety screening rates more than a brief sleep-hygiene handout among Norwegian general-practice patients prescribed zopiclone or zolpidem.
Key Findings
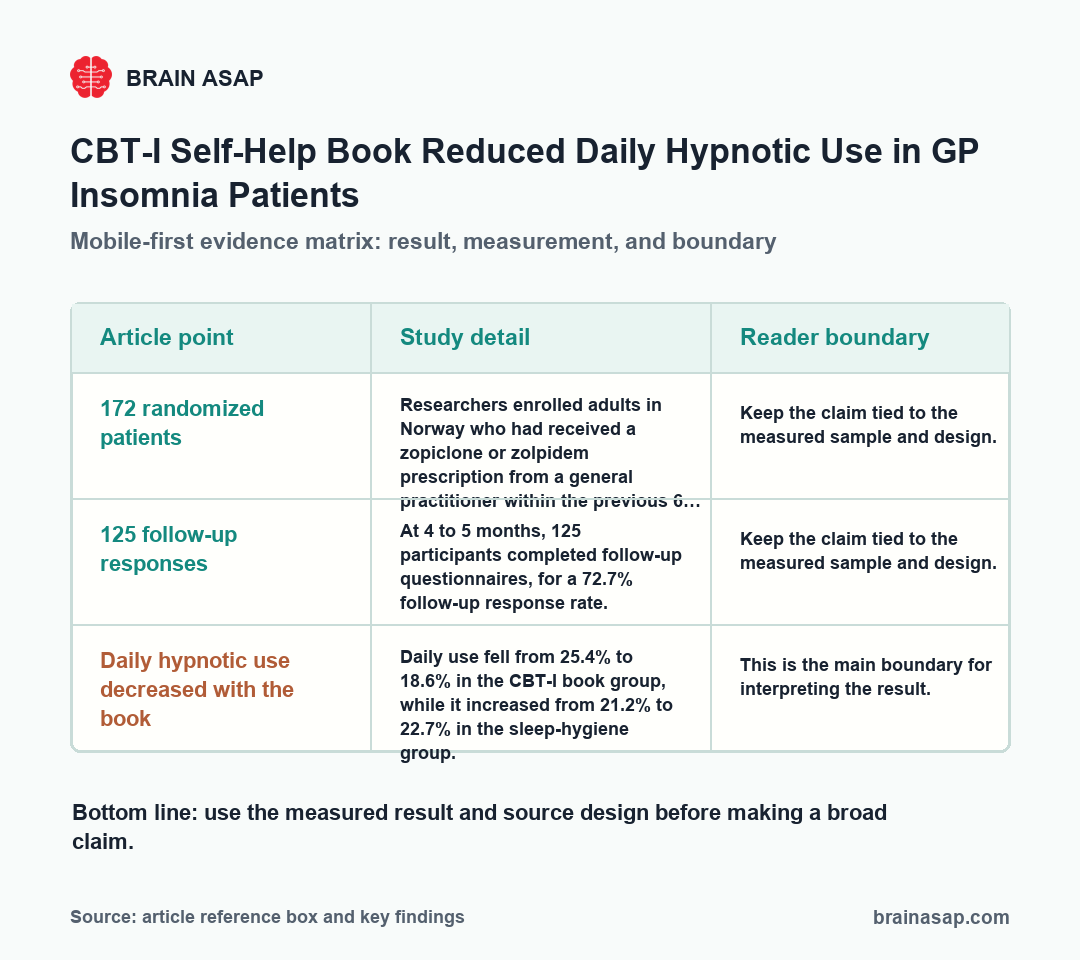
- 172 randomized patients: Researchers enrolled adults in Norway who had received a zopiclone or zolpidem prescription from a general practitioner within the previous 6 months, assigning 86 to sleep hygiene advice and 86 to the CBT-I self-help book.
- 125 follow-up responses: At 4 to 5 months, 125 participants completed follow-up questionnaires, for a 72.7% follow-up response rate.
- Daily hypnotic use decreased with the book: Daily use fell from 25.4% to 18.6% in the CBT-I book group, while it increased from 21.2% to 22.7% in the sleep-hygiene group.
- Anxiety screening improved directionally: Patient Health Questionnaire-4 anxiety-screen positivity decreased from 32.1% to 23.2% with the book and increased from 27.0% to 31.7% with sleep hygiene advice.
- Insomnia symptoms improved in both groups: Insomnia Severity Index scores decreased significantly in both arms, so the trial did not show a clear between-group advantage for insomnia symptom score.
- Sleep duration increased only in the book group: Reported sleep duration increased from 343 to 365 minutes in the CBT-I book group, while the sleep-hygiene group changed from 347 to 357 minutes.
Source: Scandinavian Journal of Primary Health Care (2025) | Bjorvatn et al.
CBT-I targets the habits, schedules, and sleep-related thoughts that keep insomnia going after the original trigger has faded. For people prescribed z-hypnotics, a drug class that includes zopiclone and zolpidem, long-term daily use can create tolerance, dependence, and a harder path away from medication-based sleep.
CBT-I Self-Help Was Tested Against Sleep Hygiene Advice
Chronic insomnia is not just a problem of too little sleep. It often involves a learned cycle in which the bed becomes linked with wakefulness, frustration, clock-watching, daytime compensation, and uneven medication use.
CBT-I, or cognitive behavioral therapy for insomnia, is designed to break that cycle. Core components include sleep restriction, stimulus control, cognitive techniques, relaxation methods, and basic sleep hygiene.
The active ingredients are usually more specific than general advice to avoid caffeine late in the day or keep the bedroom quiet.
Researchers compared two written interventions that a general-practice clinic could realistically send to patients:
- Sleep-hygiene handout: One group received a brief advice sheet covering caffeine, nicotine, alcohol as a sleep aid, heavy meals before bed, late exercise, and bedroom conditions.
- 187-page CBT-I book: The other group received the Norwegian self-help book Better Sleep. which explains sleep regulation, insomnia assessment, causes of poor sleep, and a CBT-I treatment program.
- Access question: The comparison tested whether structured self-help could do more than the kind of short sleep-hygiene advice that is easy to hand out in primary care.
A self-help book sits between two common options: more structured than a handout, less resource-intensive than specialist-delivered CBT-I.
Norwegian GP Patients Had Recent Zopiclone or Zolpidem Prescriptions
The trial used PraksisNett, a Norwegian general-practice research network. Participating general practitioners identified adults who had been prescribed zopiclone or zolpidem in the past 6 months and invited them through Norway’s digital health portal.
The flow from invitation to follow-up gives the result its practical context:
- 455 invitations: General practitioners sent digital invitations to eligible patients through Norway’s health portal.
- 172 randomized patients: A total of 197 patients consented, and 172 provided the contact information needed to receive written material.
- 125 follow-up responders: At 4 to 5 months, 125 participants completed follow-up questionnaires, a 72.7% follow-up response rate.
- Primary-care burden: About 35% were 65 or older, 69% were female, and many reported chronic medical conditions such as hypertension, neurological disease, cardiovascular disease, cancer, sleep apnea, or rheumatic disease.
Sleep problems were usually long-running. Nearly 70% reported sleep problems lasting more than 5 years, and 83.1% met criteria for insomnia on the Insomnia Severity Index, a seven-item questionnaire used to rate insomnia symptoms and severity.
Daily sleep-medication use was less common than the prescription history might imply. At baseline, 26.7% of the randomized sample reported daily prescribed sleep-medication use, while most reported less-than-daily use.
The CBT-I Book Reduced Daily Hypnotic Use More Than Sleep Hygiene
The main medication result favored the CBT-I book: among follow-up responders, daily hypnotic use fell from 25.4% to 18.6% in the book group, while daily use in the sleep-hygiene group moved from 21.2% to 22.7%.
The medication result is easiest to read as three linked findings:
- Main daily-use comparison: Daily hypnotic use fell in the CBT-I book group and rose slightly in the sleep-hygiene group.
- Primary mixed model: The generalized linear mixed model produced p = 0.077 for the time-by-group effect, with a very wide confidence interval, so this primary test was suggestive rather than conventionally significant.
- Supportive sensitivity analysis: The penalized quasi-likelihood model favored the book, with odds ratio 6.69, 95% confidence interval 2.30 to 19.47, and p = 0.001.
- Weekly-use frequency: Days per week with hypnotic use decreased significantly only in the book group, from 3.5 to 2.8 days per week.
The clinical reading should stay narrow. The trial supports a low-threshold tool that may help some prescribed hypnotic users reduce daily use; it does not show that a book can replace clinician-guided CBT-I for everyone with chronic insomnia.
Insomnia Scores Improved in Both Arms, But Anxiety Favored the Book
The other outcomes separated into a more nuanced pattern:
- Insomnia Severity Index: Scores improved significantly in both groups, and the time-by-group interaction was not significant. The trial did not prove that the book beat sleep hygiene advice on insomnia symptom score.
- Sleep duration: Reported sleep duration increased from 343 to 365 minutes in the CBT-I book group, a significant within-group change. The sleep-hygiene group changed from 347 to 357 minutes, and the between-group interaction was not significant.
- PHQ-4 anxiety screen: The Patient Health Questionnaire-4, or PHQ-4, is a four-question screen for anxiety and depressive symptoms. Anxiety-screen positivity decreased from 32.1% to 23.2% in the book group and increased from 27.0% to 31.7% in the sleep-hygiene group, with a significant time-by-group interaction.
- Depression screen: PHQ-4 depression-screen positivity stayed close to baseline in both arms, and total anxiety and depression scores did not show significant between-group effects in the continuous analyses.
The medication and anxiety results fit a plausible mechanism. A structured CBT-I program can give patients more tools for handling wakefulness without immediately relying on a pill, and reduced nighttime helplessness may also reduce anxiety for some people.
Why a Book Could Beat a One-Page Insomnia Handout
Sleep hygiene advice is easy to deliver, but it often stops at environmental and behavioral tips. Those tips can help some people, but chronic insomnia commonly needs a stronger reset of time in bed, sleep pressure, conditioned arousal, and the thoughts that make wakefulness escalate.
The book included sleep restriction, one of the best-supported CBT-I components. In CBT-I, sleep restriction matches time in bed more closely to actual sleep time, then gradually expands time in bed as sleep efficiency improves.
It also included stimulus control, which trains the bed and bedroom to function as cues for sleep rather than cues for lying awake.
That can mean leaving the bedroom temporarily when sleep does not come after a short period, avoiding wakeful activities in bed, and keeping rise time stable.
Those details matter because chronic insomnia often persists through patterns that ordinary advice does not reach:
- Extended time in bed: People may spend more hours in bed to compensate for poor sleep, but that can weaken sleep pressure and increase wakeful frustration.
- Conditioned arousal: Repeated wakefulness in bed can train the sleep environment to trigger alertness rather than sleep readiness.
- Medication confidence: A structured plan may make it easier to reduce daily hypnotic use without feeling abandoned.
- Accessible delivery: A book cannot personalize care like a clinician, but it can deliver more treatment logic than a brief handout.
Participant feedback also leaned toward the book. Satisfaction was reported by 48.2% of the book group compared with 36.5% of the sleep-hygiene group, and 58.9% of the book group said they followed the advice compared with 52.4% of the sleep-hygiene group.
The Insomnia Trial Supports Access, Not Self-Treatment for Everyone
The trial has several limits that should shape interpretation:
- Questionnaire follow-up: Medication use, sleep duration, and symptoms came from online questionnaires rather than objective dispensing records or actigraphy.
- Follow-up attrition: Of 172 randomized participants, 125 completed follow-up, so the result depends on people who remained reachable and willing to answer after 4 to 5 months.
- No usual-care-only arm: Both groups received written material, and both insomnia scores improved, so the trial mainly compares two low-intensity written approaches.
- Norwegian-language material: The sample came from Norwegian primary care and required enough Norwegian fluency to use the self-help book.
- Royalty disclosure: Bjorvatn was an author of the self-help book and reported receiving royalties, while group assignment was masked until the statistical analyses were conducted.
For clinical practice, the result supports a practical middle step. A CBT-I self-help book may help some general-practice patients reduce daily hypnotic use, especially when full CBT-I is not available quickly.
Patients with severe insomnia, high psychiatric risk, complex sleep disorders, or difficulty applying self-help instructions still need clinician-guided care.
The strongest use of the finding is not “read a book instead of getting treatment”; it is that structured CBT-I content may be worth offering earlier than many primary-care systems currently do.
Citation: DOI: 10.1080/02813432.2025.2525423. Bjorvatn et al. A randomized controlled trial comparing sleep hygiene advice with a self-help book focusing on cognitive behavioral therapy for insomnia: a study among patients with prescribed hypnotics from the GP. Scandinavian Journal of Primary Health Care. 2025;44(1):1-10.
Study design: Blinded randomized controlled trial comparing a sleep-hygiene advice sheet with a CBT-I self-help book, with 4- to 5-month questionnaire follow-up.
Sample Size: 172 Norwegian general-practice patients prescribed zopiclone or zolpidem within the previous 6 months; 125 completed follow-up.
Key Statistic: Daily hypnotic use fell from 25.4% to 18.6% in the CBT-I book group and increased from 21.2% to 22.7% in the sleep-hygiene group.
Caveat: Medication use and symptoms were questionnaire-reported, and follow-up covered 4 to 5 months.