TL;DR: A 2026 randomized trial in Archives of Disease in Childhood: Fetal and Neonatal Edition found that extended caffeine therapy reduced intermittent hypoxia, brief repeated oxygen-desaturation episodes, in very preterm infants through 41 weeks postmenstrual age.
Key Findings
- 160 infants randomized: The ICAF trial assigned 78 infants to placebo and 82 infants to extended caffeine after routine caffeine treatment would usually stop.
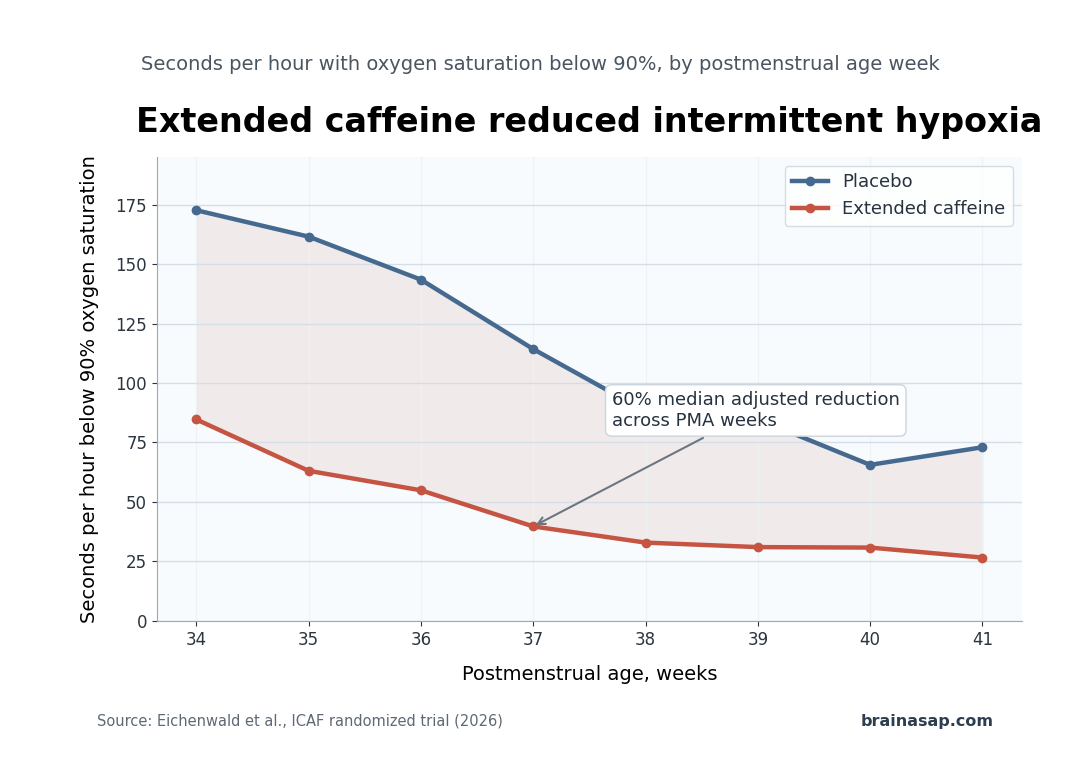
- Less intermittent hypoxia: Caffeine-treated infants had fewer seconds per hour with oxygen saturation below 90% from 34 through 41 weeks postmenstrual age.
- Median 60% reduction: Across postmenstrual-age weeks, the adjusted reduction in hypoxia burden was large, with individual weeks ranging from 42% to 65% lower.
- TNF-alpha was 23% lower: One inflammatory biomarker, tumor necrosis factor alpha, was lower at follow-up in the caffeine group after adjustment.
- No MRI signal detected: Paired brain MRI, diffusion imaging, and spectroscopy did not show significant treatment-group differences, partly because scan numbers were limited.
Source: Archives of Disease in Childhood: Fetal and Neonatal Edition (2026) | Eichenwald et al.
Very preterm infants often receive caffeine early in neonatal care because caffeine helps treat apnea of prematurity. Routine treatment usually ends around the mid-30-week postmenstrual-age window, before immature breathing control has fully settled.
The ICAF trial tested a practical extension of that familiar treatment. Researchers asked whether continuing caffeine through 42 completed weeks postmenstrual age would reduce intermittent hypoxia, the repeated dips in oxygen saturation that can persist after routine caffeine is stopped.
Extended Caffeine Reduced Oxygen Desaturation Time
Researchers enrolled infants born at 30 weeks plus 6 days of gestation or earlier who were still receiving caffeine between 32 and 36 weeks postmenstrual age, were in room air, and would normally stop caffeine before 36 weeks plus 6 days.
Randomization happened after routine caffeine was discontinued. Infants received either placebo or caffeine base at 5 mg/kg/day, later increased to twice-daily dosing, with weekly weight adjustment until the study drug ended.
- Trial design: Multicenter, masked, randomized placebo-controlled trial across 16 U.S. hospitals.
- Treatment window: Study drug continued through 42 weeks plus 6 days postmenstrual age.
- Main measurement: High-resolution pulse oximetry tracked seconds per hour with oxygen saturation below 90%.
- Analysis group: 160 randomized infants contributed to the main comparison after 10 infants withdrew before randomization.
The main result was consistent. From 34 through 41 weeks, infants assigned to caffeine spent less time below the 90% oxygen-saturation threshold at every measured postmenstrual-age week.
At 34 weeks, the placebo group averaged 172.7 seconds per hour below 90% oxygen saturation, compared with 84.7 seconds per hour in the caffeine group. At 41 weeks, the comparison was 73.0 vs 26.6 seconds per hour.
The Oxygen Effect Was Large Across Several Weeks
The adjusted percent difference favored caffeine at each postmenstrual-age week from 34 through 41 weeks. The median reduction was 60%, with the smallest adjusted weekly reduction at 42% and the largest at 65%.
Oxygen-saturation thresholds below 85% and below 80% showed similar decreases, suggesting the treatment effect was not limited to the mildest desaturation category.
- 34 weeks: Caffeine was associated with a 49% lower geometric mean time below 90% oxygen saturation.
- 37 weeks: The adjusted reduction reached 65%, with placebo infants averaging 114.3 seconds per hour below 90% and caffeine infants averaging 39.7.
- 40 weeks: The adjusted reduction was 51%, with 65.6 seconds per hour in placebo and 30.8 in caffeine.
- 41 weeks: The adjusted reduction was 64%, with 73.0 seconds per hour in placebo and 26.6 in caffeine.
Salivary caffeine levels in the caffeine group were in the therapeutic range during both sampling periods. The trial was testing continued caffeine exposure, not just assignment to a medication bottle.
TNF-Alpha Fell, but Brain Imaging Did Not Separate the Groups
Researchers also measured inflammation-related plasma biomarkers and brain imaging markers. The clearest biomarker result involved TNF-alpha, an inflammatory signaling protein also called tumor necrosis factor alpha.
Paired plasma samples were available for 62 placebo and 71 caffeine infants overall. For TNF-alpha specifically, the adjusted follow-up level was 23% lower in the caffeine group compared with placebo.
Other measured plasma biomarkers did not differ significantly after adjustment. The inflammatory result was therefore narrower than a broad anti-inflammatory signature.
- Primary oxygen result: Strong and consistent across postmenstrual-age weeks.
- Biomarker result: Limited mainly to TNF-alpha, with no significant differences across the other measured biomarkers.
- Brain imaging result: No significant MRI, diffusion, or spectroscopy differences after correction for multiple comparisons.
The imaging arm had a smaller usable sample than the oxygen-monitoring arm. Researchers completed 88 MRIs, but only 59 paired MRIs were successfully analyzed, with fewer usable scans for some volume, diffusion, and spectroscopy measures.
Clinical Signals Need a Larger Trial
Exploratory clinical results also favored caffeine in some areas. Fewer caffeine-treated infants restarted supplemental oxygen, with 4 vs 14 infants in caffeine and placebo groups.
Median time from randomization to discharge was also shorter, at 17 vs 27 days.
Those signals should be read carefully. The trial stopped below its planned sample size because of loss of funding, and the discharge findings were not the main pre-specified endpoint.
- Safety: Researchers reported no clinically important differences in adverse events, adverse events of special interest, study-drug-related adverse events, serious adverse events, or sleep-quality measures.
- Growth: Caffeine-treated infants had slower mean daily weight gain before discharge, 27.0 vs 32.1 grams per day.
- Power: Enrollment was smaller than planned, reducing the ability to detect smaller or more variable effects.
- Long-term outcomes: The study did not prove that reducing intermittent hypoxia improves later neurodevelopment.
The clinical interpretation is therefore specific: extended caffeine reduced intermittent hypoxia in very preterm infants during the late postmenstrual-age period when desaturation can still persist.
Whether that oxygen improvement translates into better long-term developmental outcomes needs a larger follow-up trial.
Citation: DOI: 10.1136/archdischild-2025-329230. Eichenwald et al. Intermittent Hypoxia and Caffeine in Infants Born Preterm: The ICAF Randomized Trial. Archives of Disease in Childhood: Fetal and Neonatal Edition. 2026;111:F249-F255.
Study Design: Multicenter masked randomized placebo-controlled trial at 16 U.S. hospitals.
Sample Size: 160 randomized very preterm infants, with 78 assigned to placebo and 82 assigned to extended caffeine.
Key Statistic: Extended caffeine reduced seconds per hour below 90% oxygen saturation from 34 through 41 weeks postmenstrual age, with a median adjusted reduction of 60%.
Caveat: The trial was smaller than planned and did not show whether reduced intermittent hypoxia improves long-term neurodevelopment.