TL;DR: A 2026 real-world cohort study in Journal of Diabetes & Metabolic Disorders linked GLP-1 receptor agonists, drugs targeting a glucose-related metabolic hormone pathway, to a higher hazard of new hypersomnolence, but the absolute risk increase was small.
Key Findings
- 237,986 matched patients: The TriNetX analysis compared 118,993 GLP-1 receptor agonist users with 118,993 matched non-users.
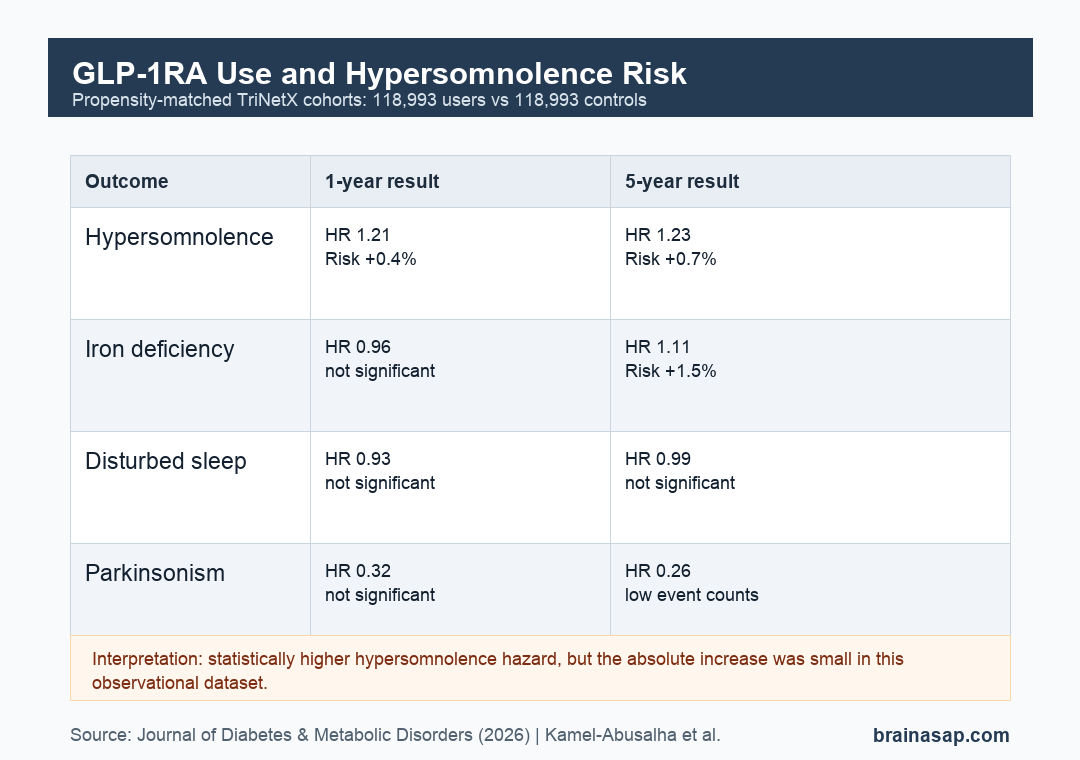
- Hypersomnolence hazard increased: GLP-1RA use was associated with hypersomnolence at 1 year (HR 1.21, 95% CI 1.10-1.32) and 5 years (HR 1.23, 95% CI 1.14-1.32).
- Absolute risk stayed modest: The cumulative risk difference was about 0.4% at 1 year and 0.7% at 5 years.
- Iron deficiency rose at 5 years: The 5-year hazard ratio for iron deficiency was 1.11 (95% CI 1.06-1.16), with a 1.5% absolute risk difference.
- Other sleep outcomes were not confirmed: Time-to-event analyses did not show significant associations for parasomnia, disturbed sleep, restless legs syndrome, or narcolepsy/cataplexy.
Source: Journal of Diabetes & Metabolic Disorders (2026) | Kamel-Abusalha et al.
GLP-1RA Sleep Risk Was Tested in a Matched Cohort
GLP-1 receptor agonists (GLP-1RAs) are drugs used for type 2 diabetes and obesity. Semaglutide and liraglutide are examples from a drug class now used by a large and growing patient population.
The study asked whether GLP-1RA exposure was associated with hypersomnolence, meaning new coded hypersomnia or somnolence, in people with obesity or type 2 diabetes who had undergone polysomnography.
Polysomnography was used as a cohort-selection strategy, not as proof that every patient had a specific sleep disorder. The goal was to enrich the dataset for people already being evaluated for sleep-related symptoms.
Researchers excluded patients with prior antidepressant use to reduce confounding from centrally acting drugs. They also excluded anyone with prior history of each outcome before analyzing incident events.
118,993 GLP-1RA Users Were Matched to 118,993 Controls
The analysis used the TriNetX Research Network, a large electronic health record dataset. Before matching, the database query identified 173,446 GLP-1RA users and more than 2.6 million controls.
After 1:1 propensity matching, each cohort included 118,993 patients. Baseline characteristics were well balanced, with standardized mean differences below 0.10 across listed covariates.
The matching model included demographics, medical conditions, and medications that could affect sleep outcomes:
- Sleep and respiratory factors: obstructive sleep apnea and related sleep evaluation context.
- Mental-health factors: mood disorders and anxiety disorders.
- Pain and medication factors: chronic pain syndrome, benzodiazepines, antihistamines, and other medication classes.
- Metabolic factors: obesity, type 2 diabetes, hyperlipidemia, chronic kidney disease, and heart failure.
Even with matching, this was still an observational study. Matching can reduce measured imbalance, but it cannot remove unmeasured differences in symptoms, adherence, dose, sleep architecture, or prescribing reasons.
Hypersomnolence Hazard Increased at 1 and 5 Years
The primary result was consistent across both follow-up windows. GLP-1RA users had a higher hazard of new hypersomnolence at 1 year and 5 years.
At 1 year, hypersomnolence occurred in 1,165 GLP-1RA users and 739 controls. The hazard ratio was 1.21, and the cumulative incidence difference was about 0.4 percentage points.
At 5 years, hypersomnolence occurred in 2,015 GLP-1RA users and 1,193 controls. The hazard ratio was 1.23, and the cumulative incidence difference was about 0.7 percentage points.
The relative and absolute results should be read together:
- Relative hazard: GLP-1RA users had about a 21-23% higher hazard of hypersomnolence.
- Absolute risk: the extra cumulative risk was less than 1 percentage point at both timepoints.
- Clinical balance: that small increase has to be weighed against metabolic and cardiovascular benefits when the drugs are otherwise indicated.
Other Sleep Outcomes Did Not Show the Same Time-to-Event Signal
The secondary outcomes were more mixed. Parasomnia had elevated cumulative risk ratios, but time-to-event analysis did not reach statistical significance.
Narcolepsy/cataplexy also did not show a significant association. Event counts were low, and confidence intervals were wide, which limits precision.
Disturbed sleep, including insomnia and related sleep codes, had non-significant hazard ratios at 1 year and 5 years. Restless legs syndrome also did not reach statistical significance in the hazard models.
Iron deficiency was the other statistically significant finding. It was not significant at 1 year, but at 5 years GLP-1RA users had a higher hazard of iron deficiency, with HR 1.11 and a 1.5 percentage-point absolute risk difference.
Brain Arousal Biology Makes the Sleep Question Plausible
The source discussed a possible mechanism involving central GLP-1 signaling. GLP-1 receptors are expressed in brain regions involved in arousal and sleep-wake regulation, including the hypothalamus and brainstem.
One proposed pathway involves orexin neurons, cells in the lateral hypothalamus that help maintain wakefulness and stabilize sleep-wake transitions. Orexin disruption is central to narcolepsy biology.
GLP-1 signaling can suppress ghrelin, a hunger-related hormone that stimulates orexin-producing neurons. The study therefore raised the possibility that GLP-1RA exposure could affect arousal through orexin-related pathways.
This remains a hypothesis. Administrative data can show associations between prescriptions and diagnostic codes, but it cannot measure orexin tone, REM sleep architecture, or objective daytime sleepiness.
Observational Coding Limits Keep the Result Cautious
The main caveat is causality. GLP-1RA users may differ from controls in ways not fully captured by diagnosis and medication codes, even after propensity matching.
Several limits shape the result:
- No patient-level symptom severity: the dataset did not provide detailed sleepiness scales or clinical narratives.
- No polysomnography metrics: sleep-stage architecture and objective sleep-test values were not used as outcomes.
- No drug-specific analysis: the study did not separate individual GLP-1RA agents, doses, duration, or adherence.
- Possible coding bias: diagnostic code errors or missed codes could misclassify outcomes.
For clinicians and patients, the practical takeaway is not that GLP-1RAs commonly cause major sleep disorders. The data suggest a small but measurable increase in coded hypersomnolence that deserves follow-up in prospective sleep studies.
Citation: DOI: 10.1007/s40200-026-01929-0. Kamel-Abusalha et al. Association of GLP-1 Receptor Agonist Use with Hypersomnolence: A Real-world Cohort Analysis. Journal of Diabetes & Metabolic Disorders. 2026;25:117.
Study Design: Retrospective propensity-matched real-world cohort analysis using the TriNetX Research Network.
Sample Size: 118,993 GLP-1RA users and 118,993 matched non-users with obesity or type 2 diabetes who underwent polysomnography.
Key Statistic: GLP-1RA use was associated with hypersomnolence at 1 year (HR 1.21, 95% CI 1.10-1.32) and 5 years (HR 1.23, 95% CI 1.14-1.32).
Caveat: Observational diagnosis-code data cannot prove causality or distinguish specific GLP-1RA drugs, doses, adherence, or objective sleep-test changes.





