
TL;DR: A 2026 systematic review and meta-analysis in Psychogeriatrics linked loneliness with Alzheimer’s disease and several forms of suicidal behavior, with especially strong shared correlations for hopelessness, insomnia, entrapment, and stress.
Key Findings
- 316 studies reviewed: Researchers found 44 studies on loneliness and Alzheimer’s disease, 261 on loneliness and suicide, and no original study that directly tested all three together.
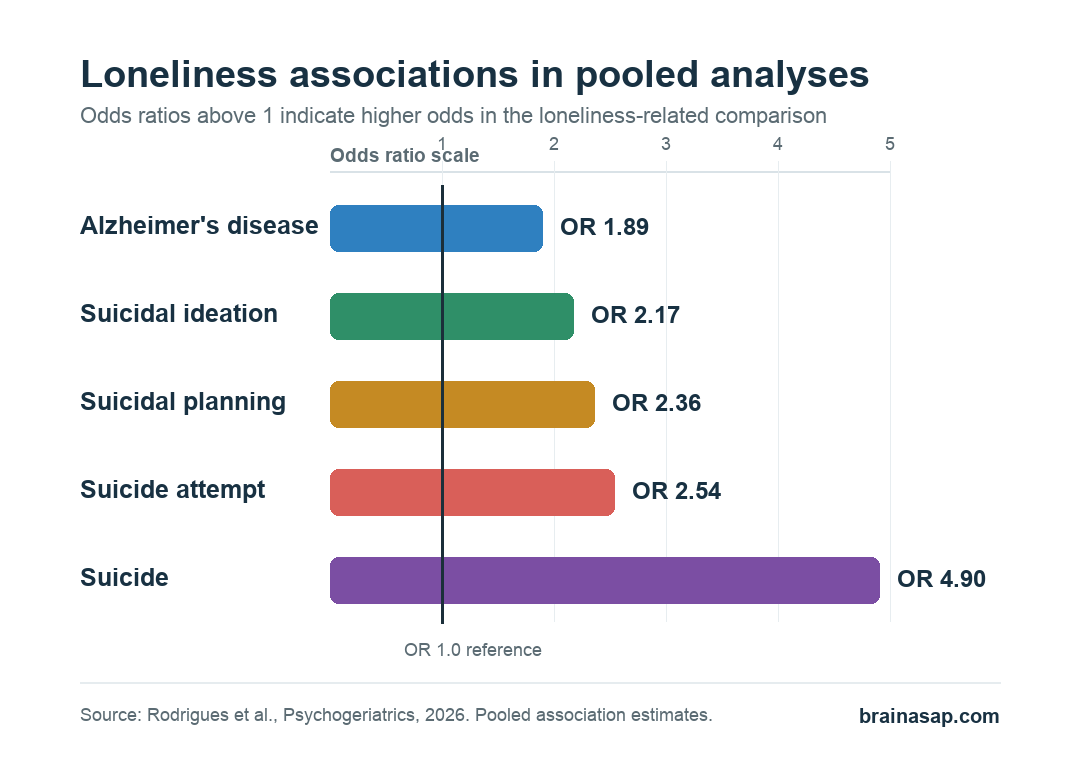
- Alzheimer’s association: Loneliness was associated with Alzheimer’s disease in pooled analyses, including an odds ratio (OR) of 1.89.
- Suicidal behavior association: Loneliness was associated with suicidal ideation, planning, attempts, and suicide, with pooled ORs ranging from 2.17 to 4.90.
- Shared distress profile: Hopelessness, insomnia, entrapment, and stress showed correlations above 0.40 with the combined Alzheimer’s and suicidality factor.
- Main caveat: The review pooled very different study designs and cultures, so the estimates should not be read as one universal risk number.
Source: Rodrigues et al. reviewed loneliness as a possible bridge between Alzheimer’s disease and suicidal behavior, then combined meta-analysis with meta-analytic factor analysis, a method that looks for shared correlation patterns across published studies.
Loneliness is often discussed as a social problem. This review treated it as a measurable mental-health and brain-health marker, then asked whether the same loneliness-related distress factors appear in two high-risk areas: Alzheimer’s disease and suicidal behavior.
The important point is not that loneliness by itself diagnoses either condition. The useful result is narrower: across a large body of published work, loneliness repeatedly appeared beside cognitive decline, Alzheimer’s disease, suicidal ideation, suicidal planning, suicide attempts, and suicide.
Researchers Found Separate Literatures, Not a Direct Three-Way Study
The review started from two parallel searches. One covered loneliness and Alzheimer’s disease; the other covered loneliness and suicidal behavior.
Researchers searched multiple databases, including PubMed, Embase, Lilacs, Ichushi, CNKI, Wanfang, and VIP.
That broad search identified 3578 articles. After screening and full-text review, the final evidence base included 316 studies.
- Alzheimer’s disease and loneliness: 44 studies covered this relationship.
- Suicide and loneliness: 261 studies covered this relationship.
- Direct overlap: no original study tested loneliness, Alzheimer’s disease, and suicidal behavior in the same analysis.
This gap changes the interpretation. The paper is not reporting a single prospective cohort where loneliness predicted both Alzheimer’s disease and later suicide outcomes in the same people.
Instead, it synthesizes two adjacent research areas and then looks for shared factors that repeatedly appear in both.
Loneliness Was Associated With Alzheimer’s Disease in Pooled Data
For Alzheimer’s disease, the pooled association depended on the type of estimate used. Four studies measured cumulative risk of Alzheimer’s disease in people who experienced loneliness, giving a pooled risk ratio of 1.64 with low heterogeneity.
Three studies measured immediate or time-to-event risk, giving a pooled hazard ratio of 1.49. When researchers pooled Alzheimer’s disease and loneliness as an odds-ratio comparison, the estimate was OR 1.89.
- Risk ratio: loneliness was linked with higher cumulative Alzheimer’s disease risk across included studies.
- Hazard ratio: loneliness was linked with higher time-to-event Alzheimer’s disease risk.
- Odds ratio: Alzheimer’s disease and loneliness were associated, but this pooled estimate had very high heterogeneity.
The heterogeneity warning is not a side issue. The Alzheimer’s odds-ratio analysis combined studies that differed in design, population, measurement, and cultural setting.
A stronger reading is that loneliness belongs on the risk-and-care radar in Alzheimer’s research, not that one pooled number should be used for individual prediction.
Suicidal Behavior Associations Were Larger but Highly Variable
The suicide side of the review was much larger. For suicidal ideation alone, researchers pooled 66 cohort and cross-sectional studies. The overall association between loneliness and suicidal ideation was OR 2.17.
Other suicidal behavior outcomes showed similar or larger associations. Suicidal planning was associated with loneliness at OR 2.36, and suicide attempts at OR 2.54. A case-control estimate for suicide was OR 4.90.
- Suicidal ideation: pooled OR 2.17, with high heterogeneity.
- Suicidal planning: pooled OR 2.36, also with high heterogeneity.
- Suicide attempt: pooled OR 2.54, with high heterogeneity and possible bias by Egger’s test.
- Suicide: OR 4.90 in the case-control evidence highlighted by the review.
These are association estimates, not proof that loneliness directly causes suicidal behavior. Clinically, the pattern points to loneliness as a marker that may travel with depression, insomnia, hopelessness, perceived burdensomeness, and social disconnection.
Hopelessness and Insomnia Stood Out in the Shared Factor Analysis
The paper also used meta-analytic factor analysis to look for factors that clustered with loneliness across the Alzheimer’s disease and suicidality interface. In that matrix, the strongest correlation with the combined disease/suicidality factor was hopelessness at 0.628.
Several other distress variables crossed the paper’s practical threshold of 0.40. Insomnia correlated with the combined factor at 0.519, entrapment at 0.466, and stress at 0.474.
- Hopelessness: the highest shared correlation in the table.
- Insomnia: a sleep-disturbance signal that also correlated with entrapment.
- Entrapment: a feeling of being unable to escape a situation or state.
- Stress: a broad distress factor that correlated with anxiety and perceived burdensomeness.
Depression remained central in the review’s narrative, but the factor table makes the practical screen broader than depression alone. In older adults, especially those with cognitive decline or Alzheimer’s disease, loneliness may warrant questions about sleep disruption, hopelessness, feeling trapped, and suicide risk.
Age, Sex, Culture, and Study Design Limit the Estimate
The review’s strength is breadth. It included work across languages, designs, and populations.
That breadth also creates the main limitation: loneliness, suicidal behavior, and Alzheimer’s disease are not measured the same way across studies.
Researchers noted that age and sex data were not explored in enough depth. Cultural context also matters because loneliness and suicidal behavior are experienced, reported, and measured differently across settings.
Practical takeaway: loneliness should not be treated as a soft background variable in Alzheimer’s care or suicide prevention. It is a measurable warning sign, but it needs to be interpreted with the person’s cognition, mood, sleep, social support, and immediate safety risk.
Citation: DOI: 10.1111/psyg.70165. Rodrigues et al. Loneliness as an Interface Between Alzheimer’s Disease and Suicidal Behaviour: A Systematic Review, Meta-Analysis and Meta-Analytic Factor Analysis. Psychogeriatrics. 2026;26:e70165.
Study Design: Systematic review, meta-analysis, and meta-analytic factor analysis of loneliness in relation to Alzheimer’s disease and suicidal behavior.
Sample Size: 316 included studies after screening 3578 records; 44 studies covered Alzheimer’s disease and loneliness, and 261 covered suicide and loneliness.
Key Statistic: Loneliness was associated with Alzheimer’s disease (OR 1.89), suicidal ideation (OR 2.17), suicidal planning (OR 2.36), suicide attempt (OR 2.54), and suicide (OR 4.90).
Caveat: No original study directly tested loneliness, Alzheimer’s disease, and suicidal behavior together, and several pooled suicide analyses had high heterogeneity.





