TL;DR: A 2026 medRxiv preprint found that giving intravenous thrombolysis (IVT), a clot-dissolving drug treatment, before endovascular thrombectomy (EVT), a catheter procedure to remove a large brain clot, did not significantly improve 3-month recovery or increase bleeding risk in selected stroke patients treated 6 to 24 hours after symptoms began.
Key Findings
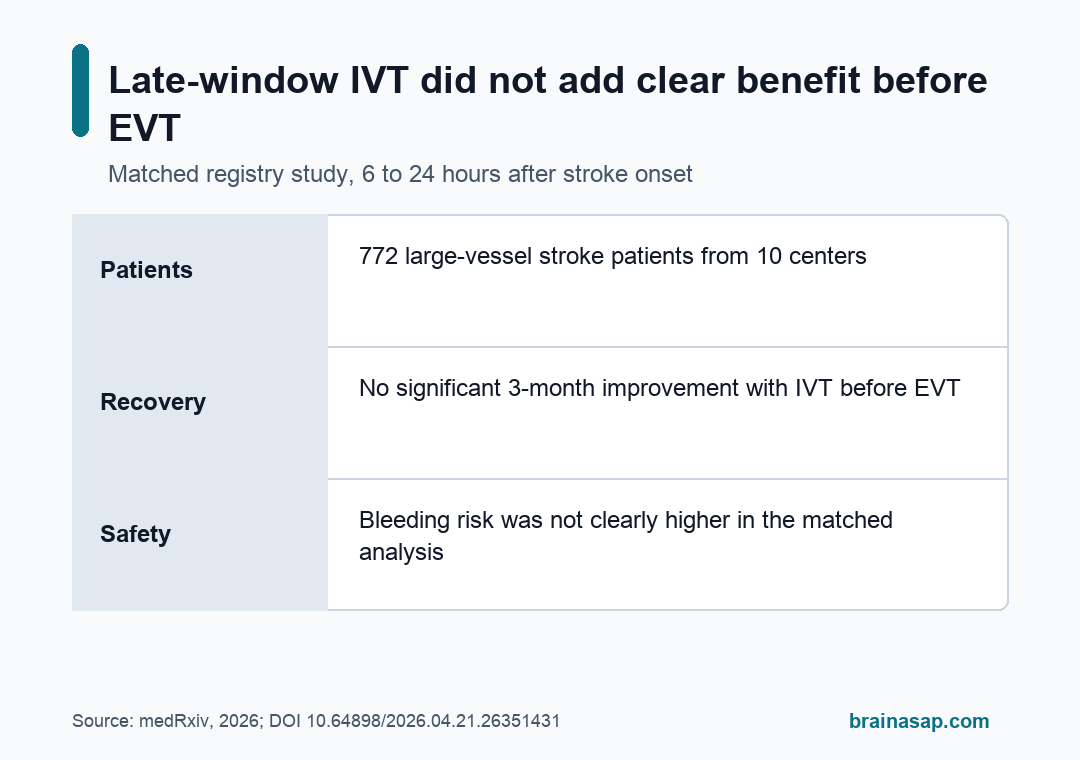
- Registry cohort: The analysis included 772 acute ischemic stroke patients from 10 comprehensive stroke centers in China and Singapore between 2019 and 2024.
- Matched comparison: Researchers matched 101 patients who received IVT plus EVT with 202 patients who received direct EVT alone, balancing baseline covariates to an absolute standardized mean difference below 0.10.
- No 3-month recovery advantage: Favorable functional outcome, defined as modified Rankin Scale (mRS) 0-2, was 44.55% with bridging IVT plus EVT versus 47.03% with direct EVT.
- No clear recanalization difference: Successful reperfusion, defined as mTICI 2b-3, was 91.09% with bridging treatment versus 90.10% with direct EVT.
- No significant bleeding penalty: Symptomatic intracranial hemorrhage was 5.94% with bridging IVT plus EVT versus 9.41% with direct EVT, with a confidence interval too wide to claim protection.
Source: medRxiv (2026) | Chen et al.
Late-window stroke treatment creates a practical decision for emergency teams: if a patient is already heading for catheter-based clot removal, should clinicians also give clot-dissolving medication first?
The Chen preprint examined that uncertainty in patients with anterior-circulation large vessel occlusion, the kind of major ischemic stroke where a blocked large artery can rapidly injure brain tissue.
Late-Window Stroke Patients Had Large Vessel Occlusion
Endovascular thrombectomy (EVT) changed acute stroke care because it can reopen blocked large brain arteries by physically removing a clot. Modern stroke imaging also allows selected patients to receive EVT beyond the earliest treatment window, including some patients treated up to 24 hours after symptoms began.
Intravenous thrombolysis (IVT) is different. It is a drug-based approach that aims to dissolve clot material through the bloodstream.
In standard early stroke windows, many patients who are eligible for both treatments receive IVT before EVT, often called bridging treatment.
Giving IVT before EVT could help by softening the clot, restoring some distal blood flow, or improving tiny downstream vessels before the catheter reaches the blockage.
It could also add bleeding risk, delay the procedure, or provide little extra value once thrombectomy is already planned.
Researchers focused on patients with anterior circulation large vessel occlusion treated in the 6- to 24-hour window.
Eligibility required EVT, Alberta Stroke Program Early CT Score (ASPECTS) of at least 6, National Institutes of Health Stroke Scale (NIHSS) of at least 6, and pre-stroke modified Rankin Scale of 2 or less.
Those criteria selected patients who still had a potentially salvageable treatment profile. ASPECTS is an imaging score for early ischemic injury, and NIHSS is a neurologic severity scale used in acute stroke assessment.
Propensity Matching Compared IVT Plus EVT With Direct EVT
This was not a randomized trial. Researchers used a prospective EVT registry and then performed a retrospective comparative analysis, which means treatment assignment reflected real-world clinical decisions rather than random allocation.
That design makes confounding a central issue. Patients selected for IVT may differ from patients sent directly to EVT because of time from onset, imaging profile, clinical severity, contraindications, or local practice.
The study used 1:2 propensity score matching to reduce those baseline differences.
Before matching, 110 of 772 patients received bridging IVT plus EVT, while 662 received direct EVT.
After matching, the analytic cohort contained 101 bridging-treatment patients and 202 direct-EVT patients.
- Primary outcome: Favorable functional outcome at 3 months, defined as mRS 0-2, meaning no symptoms through slight disability but independent daily function.
- Reperfusion outcome: Successful recanalization, defined as mTICI 2b-3, meaning substantial or complete reopening of the blocked vessel territory.
- Safety outcomes: Symptomatic intracranial hemorrhage (sICH), hemorrhagic transformation, and 3-month mortality.
The matched design helps, but it does not make the groups equivalent in the way a randomized trial would. Unmeasured reasons for withholding or giving IVT could still affect the results.
That limitation is especially important in late-window care, where treatment decisions often depend on imaging, transfer logistics, contraindications, and clinician judgment that may not be fully captured in a registry.
Bridging IVT Did Not Improve 3-Month Functional Recovery
The main recovery endpoint was nearly identical. Favorable 3-month outcome occurred in 44.55% of matched patients who received IVT plus EVT and 47.03% of matched patients who received direct EVT alone.
The common odds ratio was 0.91 with a 95% confidence interval from 0.56 to 1.46.
The estimate did not show a recovery advantage for adding IVT, and the interval crossed 1.0, so the association was not statistically significant.
Successful recanalization also looked similar: 91.09% with bridging treatment versus 90.10% with direct EVT. That result weakens a simple explanation that late-window IVT meaningfully improves the chance of reopening the vessel before or during thrombectomy in this selected cohort.
Multivariable logistic regression before matching pointed in the same general direction.
After adjustment for age, onset-to-puncture time, pre-EVT ASPECTS, pre-EVT NIHSS, coronary heart disease, and atrial fibrillation, IVT was not significantly associated with favorable outcome, recanalization, bleeding, or death.
The consistency between the regression model and the matched analysis makes the null finding more credible, although both methods still depend on measured variables and cannot replace random assignment.
Bleeding and Mortality Were Not Significantly Higher With IVT
The safety result is clinically important because concern about hemorrhage is one reason teams may avoid thrombolysis in later treatment windows.
In this matched cohort, symptomatic intracranial hemorrhage occurred in 5.94% of IVT-plus-EVT patients and 9.41% of direct-EVT patients.
That does not prove IVT was safer. The odds ratio was 0.61 with a 95% confidence interval from 0.24 to 1.58, which is too imprecise to support a protective conclusion.
A narrower reading fits the data: this dataset did not show a significant bleeding increase from bridging IVT.
Hemorrhagic transformation, a broader category of post-stroke bleeding visible on imaging, was also similar at 23.76% versus 23.27%.
Mortality at 3 months was 15.84% with IVT plus EVT and 13.37% with direct EVT, again without a statistically significant difference.
- Recovery result: No evidence that bridging IVT improved the chance of mRS 0-2 recovery at 3 months.
- Procedure result: No evidence that bridging IVT improved successful recanalization in the matched comparison.
- Safety result: No statistically significant increase in symptomatic intracranial hemorrhage, hemorrhagic transformation, or death.
Retrospective Stroke Registry Data Cannot Settle the Treatment Question
The most important limitation is design. A propensity-matched registry analysis can make observational groups more comparable, but it cannot remove every reason clinicians chose one treatment path over another.
Late-window stroke selection is especially complex. Imaging patterns, collateral circulation, clot location, contraindications to thrombolysis, transfer timing, and institutional practice can influence both treatment choice and outcome.
Another limitation is source status. This is a preprint, so it had not completed peer review when posted.
The preprint notice states that the findings should not guide clinical practice, and any treatment decision still belongs inside local stroke protocols and guideline-based emergency care.
A useful next step would be a randomized late-window trial that stratifies by imaging pattern, thrombolysis eligibility, occlusion site, and transfer timing. Those details could reveal whether a narrower subgroup benefits even if the overall registry comparison did not.
In this multicenter registry, adding IVT before EVT in selected 6- to 24-hour anterior-circulation stroke patients did not show a clear efficacy advantage or a clear safety harm compared with direct EVT alone.
Randomized late-window evidence is still needed to decide whether any subgroup benefits.
Citation: DOI: 10.64898/2026.04.21.26351431. Chen et al. Safety and Efficacy of Bridging Intravenous Thrombolysis Versus Direct Endovascular Therapy in Acute Ischemic Stroke Treated in the 6- to 24-Hour Time Window: A Propensity Score-Matched Analysis. medRxiv. 2026.
Study Design: Retrospective analysis of a prospective multicenter EVT registry with 1:2 propensity score matching.
Sample Size: 772 registry patients before matching; 303 patients in the matched comparison.
Key Statistic: Favorable 3-month outcome was 44.55% with IVT plus EVT versus 47.03% with direct EVT.
Caveat: Observational preprint data cannot rule out unmeasured treatment-selection bias or replace randomized evidence.