TL;DR: A 2026 retrospective database study in Archives of Orthopaedic and Trauma Surgery found that people with major upper-extremity amputations had higher one-year rates of new mental-health diagnoses, antidepressant starts, and psychotherapy use than matched patients with minor hand or digit amputations.
Key Findings
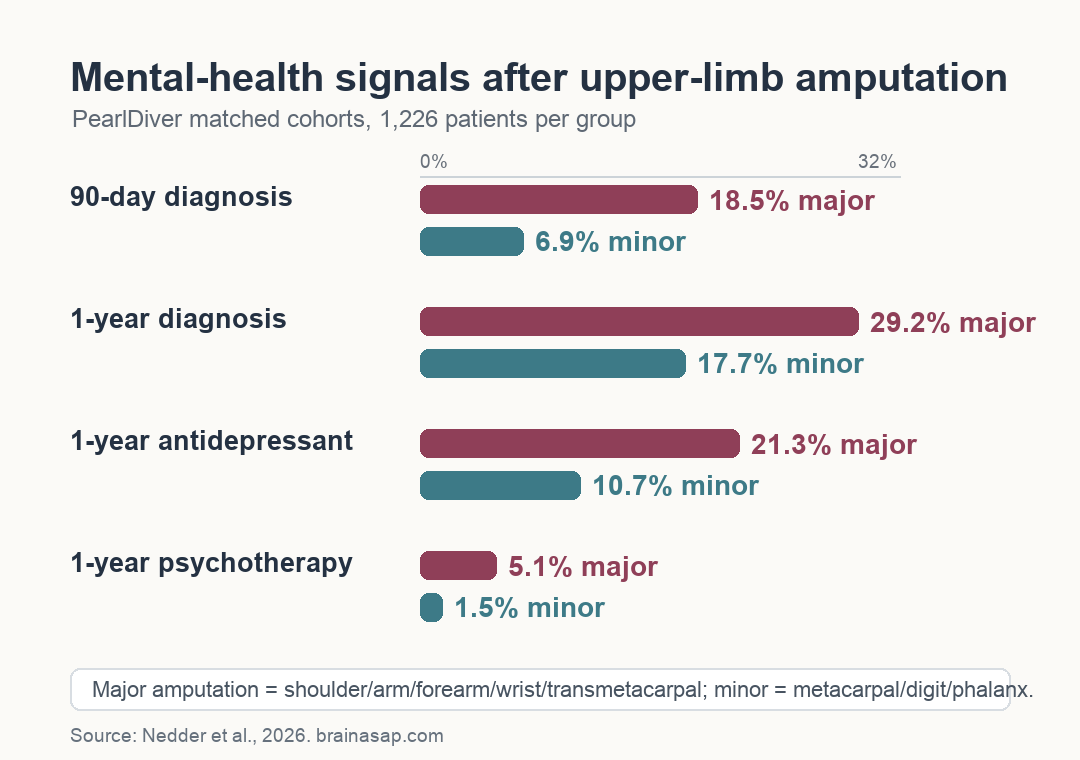
- Matched database study: Researchers compared 1,226 major upper-extremity amputation patients with 1,226 matched minor amputation patients in PearlDiver records from 2010 to 2022.
- Diagnosis gap appeared quickly: At 90 days, new mental-health diagnoses appeared in 18.5% of major amputation patients versus 6.9% of minor amputation patients.
- One-year difference persisted: By one year, the rates were 29.2% after major amputation and 17.7% after minor amputation.
- Treatment markers also differed: Major amputation was linked to higher odds of antidepressant starts and psychotherapy claims at both 90 days and one year.
- Claims data limit interpretation: The study measured diagnoses, prescriptions, and psychotherapy claims, not direct symptom interviews or unmet need.
Source: Nedder et al. 2026 Archives of Orthopaedic and Trauma Surgery study.
Upper-extremity amputation is not only a surgical and prosthetic problem. It can change work, self-care, body image, pain, daily independence, and the way a person is seen by others.
This study asked a narrower question: after upper-limb amputation, are mental-health diagnoses and treatment claims more common when the amputation is major rather than minor?
In this insurance-claims sample, major amputations were linked to higher rates of new diagnoses, antidepressant use, and psychotherapy care at both measured time points.
The result should not be read as saying minor amputations are psychologically easy. The minor-amputation group also had substantial one-year mental-health diagnoses.
The useful clinical signal is that amputation level helped identify a group with especially high follow-up needs.
Major Amputation Carried Higher One-Year Mental Health Diagnosis Rates
The researchers used the PearlDiver M170 database, a deidentified U.S. insurance-claims dataset. They identified first upper-extremity amputations from 2010 to 2022 using procedure codes.
Major amputations included shoulder disarticulation, arm, forearm, wrist, and transmetacarpal amputations. Minor amputations included single metacarpal, digit, or phalanx amputations.
The final matched sample included 2,452 patients: 1,226 in the major-amputation group and 1,226 in the minor-amputation group. Matching covered age range, sex, Elixhauser Comorbidity Index, and smoking history.
Patients were excluded if they were younger than 10, had a mental-health diagnosis or antidepressant record during the year before amputation, or lacked a full year of follow-up in the database.
The study tracked new claims for 10 mental-health diagnosis categories:
- Mood and anxiety disorders: depression, bipolar disorder, anxiety disorder, panic disorder, suicidal ideation, and suicide attempt.
- Trauma and sleep outcomes: post-traumatic stress disorder (PTSD), a trauma-related mental-health diagnosis, and sleep disorder.
- Substance-related outcomes: alcohol-related disorder and drug-related disorder excluding alcohol.
At 90 days, 18.5% of major-amputation patients had a new mental-health diagnosis compared with 6.9% of minor-amputation patients. The adjusted odds ratio was 3.29.
At one year, the gap narrowed but remained large: 29.2% after major amputation versus 17.7% after minor amputation, with an adjusted odds ratio of 2.01.
Depression, Anxiety, Sleep Disorder, and PTSD Drove the Pattern
Depression was the most common new diagnosis in the major-amputation group. Anxiety was next. In the minor-amputation group, drug-related disorder and depression were prominent, depending on the time window.
The diagnosis pattern matters because the overall category was not driven by one rare code. Several clinically recognizable outcomes stayed higher after major amputation.
The major-amputation group had higher adjusted odds for these diagnoses at one year:
- Depressive disorder: 13.1% after major amputation versus 6.3% after minor amputation; adjusted odds ratio 2.45.
- Anxiety disorder: 9.0% versus 5.4%; adjusted odds ratio 1.80.
- Sleep disorder: 5.8% versus 2.4%; adjusted odds ratio 2.71.
- PTSD: the study reported that the higher 90-day PTSD odds in major-amputation patients persisted at one year.
These are claims-based outcomes, so they depend on whether a clinician recorded the diagnosis and whether the patient had access to follow-up care.
That limitation cuts in two directions. Claims can miss distress when patients are not screened or cannot reach mental-health care. They can also reflect healthcare contact patterns rather than symptom burden alone.
Antidepressant Starts Were Also Higher After Major Amputation
The study also examined new antidepressant claims. That separate measure helps distinguish diagnosis coding from treatment starts.
At 90 days, 11.7% of major-amputation patients had started an antidepressant compared with 3.7% of minor-amputation patients. The adjusted odds ratio was 3.82.
At one year, antidepressant use reached 21.3% in the major-amputation group and 10.7% in the minor-amputation group. The adjusted odds ratio remained significant at 2.38.
The researchers counted several medication classes, including selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants, atypical antidepressants, and serotonin modulators.
SSRIs were the most used antidepressant class in both groups at both time points.
The treatment pattern supports the diagnosis pattern. Major amputation was not only linked to more coded mental-health conditions; it was also linked to more medication starts during recovery.
Psychotherapy Claims Were Low Despite Higher Diagnosis Rates
Psychotherapy claims also differed by amputation level, but the absolute percentages were small.
Psychotherapy care appeared in 3.0% of major-amputation patients and 0.7% of minor-amputation patients at 90 days, then 5.1% versus 1.5% at one year. The adjusted odds ratios were 5.47 and 4.18.
The gap is clinically important, but so is the low use. In the discussion, the researchers noted that psychotherapy use was lower than general-population estimates even though mental-health diagnoses were elevated after amputation.
That mismatch points to a possible access problem. Patients may receive a diagnosis or prescription without getting psychotherapy, or distress may go untreated when rehabilitation visits focus mainly on wound healing, prosthetics, pain, and physical function.
The paper recommended more routine mental-health resources after amputation. Practical options include screening during intake, social-work support, referral pathways, and easier access to psychology or peer support inside upper-limb rehabilitation programs.
Claims Data Cannot Measure Unmet Need Directly
The study’s main strength is scale. A matched national claims sample can capture many patients across real-world care settings, rather than a small single-center clinic sample.
The limitations are equally important:
- Retrospective design: The analysis can show associations, not prove that amputation level caused the mental-health outcomes.
- Claims dependence: Diagnoses, prescriptions, and psychotherapy only appear when they are coded or billed.
- Insured population: PearlDiver data do not represent uninsured patients, and insurance status affects access to mental-health care.
- General-population comparisons: The paper compared some rates with outside epidemiological estimates, not a perfectly matched non-amputation control group.
These limits do not erase the clinical planning problem. Major upper-extremity amputation identified a group with higher early and one-year mental-health service signals.
The practical takeaway is not that every patient needs the same psychiatric intervention. Mental-health screening should be built into upper-limb amputation recovery, especially when the amputation is major and functional disruption is likely to be high.
Citation: DOI: 10.1007/s00402-026-06319-y. Nedder et al. Analysis of mental health outcomes in major versus minor upper extremity amputations: a retrospective national database study. Archives of Orthopaedic and Trauma Surgery. 2026;146:158.
Study Design: Retrospective national insurance-claims database study with matched major and minor upper-extremity amputation cohorts.
Sample Size: 2,452 matched patients: 1,226 major amputation patients and 1,226 minor amputation patients.
Key Statistic: One-year new mental-health diagnosis rates were 29.2% after major amputation versus 17.7% after minor amputation; adjusted odds ratio 2.01.
Caveat: Claims records can miss uncoded symptoms and cannot directly measure unmet mental-health need.





