TL;DR: A 2026 study in Alzheimer’s & Dementia: Translational Research & Clinical Interventions used lecanemab pharmacokinetic/pharmacodynamic modeling in early Alzheimer’s disease and found that blood biomarkers worsened after treatment stopped, while monthly maintenance dosing after 18 months was predicted to preserve most p-tau181 and GFAP, an astrocyte-inflammation protein.
Key Findings
- Three plasma biomarkers improved: Lecanemab increased the plasma amyloid beta 42/40 ratio and decreased p-tau181 and GFAP, which track amyloid, tau-related, and astrocyte-inflammation biology in Alzheimer’s disease.
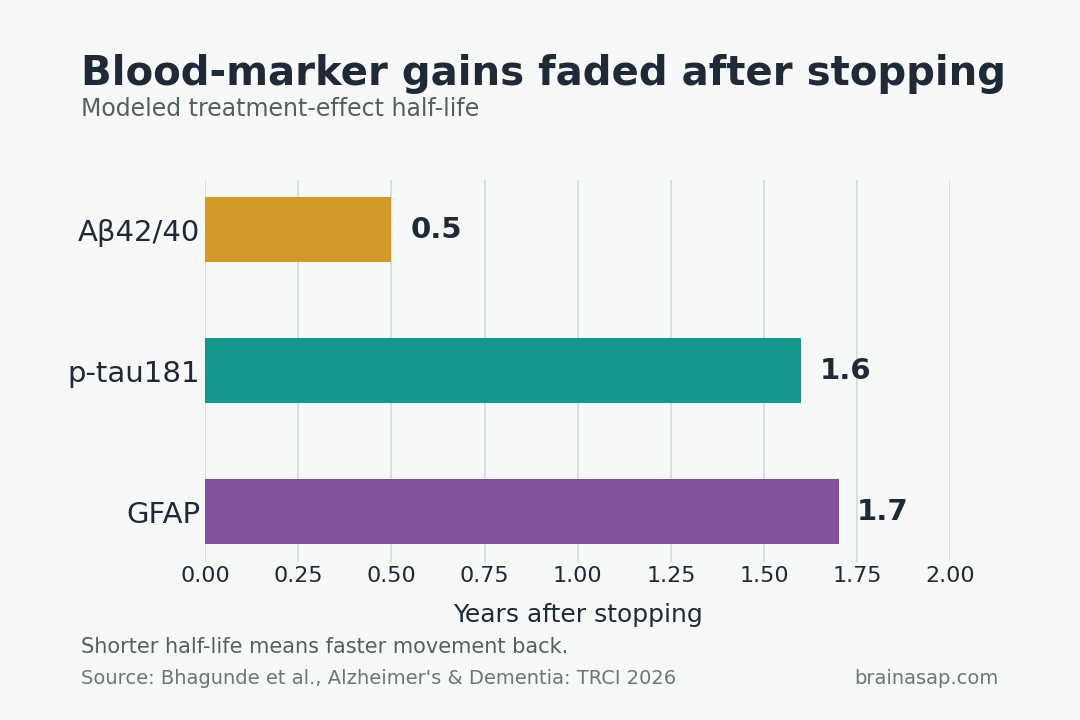
- Stopping treatment reversed blood-marker gains: After lecanemab discontinuation, the Abeta42/40 ratio lost half its treatment effect in about 0.5 years, while p-tau181 and GFAP re-accumulation half-lives were 1.6 and 1.7 years.
- Blood markers moved faster than amyloid PET: The modeled Abeta42/40 half-life was much shorter than the roughly 12.1-year half-life reported for amyloid positron emission tomography (PET) treatment-effect loss, making plasma markers more dynamic readouts.
- Monthly dosing looked sufficient after 18 months: Simulations predicted that switching from 10 mg/kg every 2 weeks to 10 mg/kg monthly at 18, 24, or 30 months maintained p-tau181 and GFAP near continuous-treatment levels.
- Early Alzheimer’s disease remains the target: The models apply best to early Alzheimer’s disease, where amyloid and early tau biology dominate; the biomarkers used here do not capture late tau pathology as well.
Source: Alzheimer’s & Dementia: Translational Research & Clinical Interventions (2026) | Bhagunde et al.
The dosing question begins after an initial infusion period, when clinicians have to decide whether to stop, continue, or step down treatment.
The analysis focused on whether blood biomarkers suggest Alzheimer’s biology stays suppressed after the first treatment phase, especially if dosing becomes less frequent.
Researchers modeled whether blood biomarkers keep improving, drift back toward baseline, or remain stable if patients move from every-2-week infusions to a less frequent monthly maintenance schedule.
Plasma Biomarkers Tracked Amyloid, Tau, and Astrocyte Biology
The analysis pooled biomarker data from the phase 2 Study 201 and phase 3 Clarity AD lecanemab programs, including core and open-label extension data. Individual lecanemab exposure was estimated with a population pharmacokinetic model, then linked to blood-marker changes with pharmacokinetic/pharmacodynamic models.
The three modeled blood markers represented different parts of Alzheimer’s pathology:
- Abeta42/40 ratio: The plasma amyloid beta 42-to-40 ratio reflects soluble and insoluble amyloid dynamics and tends to track brain amyloid biology.
- p-tau181: Plasma tau phosphorylated at threonine 181 is a tau-related marker associated with Alzheimer’s neuropathology and amyloid/tau PET stages.
- GFAP: Glial fibrillary acidic protein is an astrocyte injury and neuroinflammation marker that rises across the Alzheimer’s disease continuum.
After lecanemab treatment began, the Abeta42/40 ratio increased, while p-tau181 and GFAP decreased. Placebo participants showed worsening markers during the controlled phase, and people who later started lecanemab in the extension phase showed biomarker improvement within months.
Stopping Lecanemab Let Blood Markers Drift Back Toward Baseline
Study 201 included an interruption after 18 months of lecanemab treatment, with an average gap of about 24 months. That gap made the discontinuation pattern visible.
During the gap, biomarkers moved in the wrong direction:
- Abeta42/40 ratio decreased by 47%: The authors interpret this as renewed amyloid-related pathology after treatment stopped.
- p-tau181 increased by 24%: The tau-related plasma marker rose again during treatment interruption.
- GFAP increased by 30%: The astrocyte and neuroinflammation marker also moved back toward pretreatment biology.
The model-derived half-lives were clinically important. The Abeta42/40 treatment effect was half-lost in about 0.5 years. The corresponding estimates were 1.6 years for p-tau181 and 1.7 years for GFAP.
Amyloid PET changed much more slowly. The analysis contrasts the Abeta42/40 half-life with a reported 12.1-year amyloid PET half-life for loss of treatment effect.
The difference means blood biomarkers may warn earlier that Alzheimer’s biology is becoming active again.
Monthly Maintenance Dosing Preserved p-tau181 and GFAP
The maintenance-dose simulations tested lecanemab 10 mg/kg every 2 weeks for 18, 24, or 30 months, followed by 10 mg/kg monthly. Researchers compared those scenarios with continued every-2-week dosing through 48 months.
The simulated monthly regimen did not keep every marker identical to continuous biweekly dosing. The Abeta42/40 ratio settled at a lower plateau than the every-2-week regimen, although the authors describe that level as remaining within a range associated with amyloid negativity.
For the downstream markers, the modeled pattern was more stable. p-tau181 and GFAP stayed at levels similar to continuous biweekly treatment after the monthly switch.
The timing of the switch, between 18 and 30 months, made little difference in the 48-month profiles.
Blood Biomarkers May Help Guide Ongoing Treatment
Amyloid plaque clearance does not necessarily mean the amyloid-production process has stopped. Lecanemab binds protofibrils and plaques, with the interpretation that protofibrils can continue to be produced even after plaque levels are lowered.
In this model, ongoing treatment kept suppressing the biology that blood tests were measuring. If treatment stops after plaque clearance, blood biomarkers may begin worsening well before amyloid PET shows a large change.
Potential monitoring uses include:
- Maintenance decisions: Plasma markers may help support a move from biweekly dosing to monthly maintenance rather than full discontinuation.
- Early warning: Serial blood tests could show renewed pathology over months, not years.
- Course correction: If markers worsen during maintenance, clinicians may have a reason to reassess dosing or adherence.
The researchers also mention p-tau217 as a real-time monitoring candidate, although the actual PK/PD models used Abeta42/40, p-tau181, and GFAP.
Modeling, Sponsor Ties, and Early-Disease Scope Limit the Claim
This was a modeling and simulation study using trial-program data, not a new randomized test of monthly maintenance against discontinuation. The findings are strongest as a mechanistic and dosing-support analysis, not as direct proof that every patient should follow the same maintenance schedule.
Several boundaries matter:
- Early Alzheimer’s disease: The biomarkers are most relevant when amyloid and early tau biology are the main drivers.
- Late tau pathology: Abeta42/40, p-tau181, and GFAP do not fully capture later tau-driven disease biology.
- Industry authorship: All authors were Eisai employees, and the study was funded by Eisai and Biogen.
- Clinical outcomes: Biomarker maintenance supports the treatment rationale, but cognition and function remain the outcomes patients and clinicians care about most.
The clearest reading is that stopping lecanemab after amyloid reduction may be biologically different from stepping down to maintenance dosing. In these simulations, monthly maintenance preserved the main blood-marker gains, while discontinuation allowed Alzheimer’s-related plasma markers to re-accumulate.
Citation: DOI: 10.1002/trc2.70246. Bhagunde P et al. Pharmacokinetic/pharmacodynamic analyses of plasma pathophysiology biomarkers in subjects with early Alzheimer’s disease following lecanemab treatment. Alzheimer’s & Dementia: Translational Research & Clinical Interventions. 2026;12:e70246.
Study Design: Pharmacokinetic/pharmacodynamic modeling and simulation using pooled plasma biomarker data from lecanemab phase 2 and phase 3 early Alzheimer’s disease studies.
Sample Size: Biomarker analyses used pooled Study 201 and Clarity AD data; the population pharmacokinetic model referenced 28,116 serum lecanemab observations from 2,267 subjects.
Key Statistic: After discontinuation, modeled treatment-effect half-lives were about 0.5 years for Abeta42/40, 1.6 years for p-tau181, and 1.7 years for GFAP; amyloid PET was much slower at about 12.1 years.
Caveat: This was a sponsor-funded modeling analysis, not a direct randomized maintenance-dose outcome trial; the biomarker set fits early Alzheimer’s disease better than later tau-dominant disease.