TL;DR: A 2026 study in PLOS One found that Texas ICU COVID-19 hospitalizations coded for current nicotine dependence had lower crude and adjusted mortality than hospitalizations coded as never nicotine dependent, but the administrative-data design means the result should not be read as evidence that nicotine is protective.
Key Findings
- Large ICU cohort: Researchers analyzed 142,045 Texas ICU hospitalizations for principal-diagnosis COVID-19 from Q2 2020 through Q4 2024.
- Three exposure groups: The cohort included 10,452 current, 23,671 former, and 107,922 never nicotine-dependent hospitalizations.
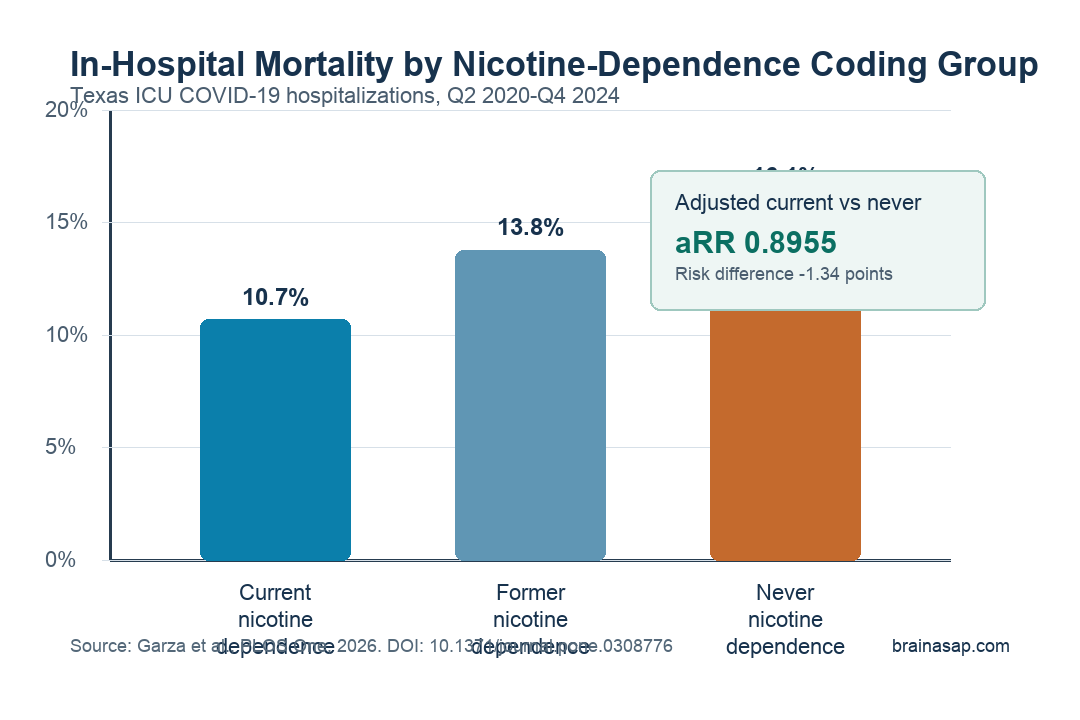
- Crude mortality was lower: In-hospital mortality was 10.7% in current nicotine dependence, 13.8% in former dependence, and 16.1% in never dependence.
- Adjustment did not erase it: Current nicotine dependence was associated with a lower adjusted in-hospital mortality risk versus never dependence, with aRR 0.8955.
- Caution is central: ICD-10 coding, repeated admissions, illness severity, treatment differences, nicotine intensity, and Texas-only data limit interpretation.
Source line: Researchers used the Texas Inpatient Public Use Data File to study adult ICU hospitalizations with principal-diagnosis COVID-19 and ICD-10-CM nicotine-dependence codes.
Nicotine dependence in this paper means a hospital billing-code category, not a direct measurement of cigarettes per day, vaping exposure, nicotine dose, or current blood nicotine level.
The distinction is important because this finding is easy to misread. The analysis does not show that nicotine helps critically ill COVID-19 patients.
It reports that, inside this administrative hospital dataset, patients coded as current or former nicotine dependent had lower mortality than patients without those codes after several adjustments.
Texas ICU Data Linked Nicotine Dependence to Lower Mortality
The study focused on adults admitted to Texas acute-care ICUs with COVID-19 listed as the principal diagnosis. Researchers excluded elective admissions, transfers, and discharges against medical advice so that the hospitalization course was more complete.
The main exposure was a three-level nicotine-dependence variable:
- Current nicotine dependence: 10,452 hospitalizations, or 7.3% of the cohort.
- Former nicotine dependence: 23,671 hospitalizations, or 16.7% of the cohort.
- Never nicotine dependence: 107,922 hospitalizations, or 76.0% of the cohort.
The crude mortality pattern ran against the researchers’ initial expectation. Current nicotine dependence had 1,115 deaths among 10,452 hospitalizations, or 10.7%.
Former nicotine dependence had 3,256 deaths among 23,671 hospitalizations, or 13.8%. Never nicotine dependence had 17,385 deaths among 107,922 hospitalizations, or 16.1%.
Short-term mortality showed the same direction: 13.5% for current nicotine dependence, 18.1% for former dependence, and 20.0% for never dependence.
Adjustment Matched Current and Never Groups More Closely
A simple crude comparison is not enough here. Nicotine-dependent patients differed from never-dependent patients in age, sex, race and ethnicity, insurance, chronic lung disease, mental disorders, substance-use diagnoses, organ dysfunction, treatment procedures, and discharge year.
The researchers used overlap weighting, a statistical approach that reweights records so the compared groups look more similar across measured covariates.
In the overlap-weighted current-versus-never comparison, both groups had the same expected values for listed covariates such as age category, insurance, comorbidities, procedures, year, and organ dysfunction count.
After that adjustment, in-hospital mortality remained lower for current nicotine dependence than never dependence: 11.4% versus 12.7% in the overlap-weighted population.
The adjusted pairwise results were:
- Current versus never: In-hospital mortality adjusted risk ratio 0.8955; short-term mortality adjusted risk ratio 0.8926.
- Current versus former: In-hospital mortality adjusted risk ratio 0.9432; short-term mortality adjusted risk ratio 0.9438.
- Former versus never: In-hospital mortality adjusted risk ratio 0.9388; short-term mortality adjusted risk ratio 0.9477.
Each adjusted risk ratio was below 1.0, meaning the nicotine-dependence group named first had lower modeled mortality risk than the comparison group. The adjusted risk differences were small in absolute terms, ranging from about 0.7 to 1.7 percentage points in the main table.
High-Risk Subgroups Kept the Same Direction
The study also tested whether the current-versus-never result held in groups with higher baseline mortality risk. It did, at least across the measured strata the paper reported.
Among hospitalizations with a Deyo comorbidity index of 3 or higher, in-hospital mortality was 11.0% in current nicotine dependence versus 19.9% in never dependence.
Among patients aged 65 or older, the rates were 12.2% versus 19.4%.
The same direction appeared in the sickest procedure-defined groups:
- Three or more organ dysfunctions: In-hospital mortality was 40.6% in current nicotine dependence and 50.5% in never dependence.
- Invasive mechanical ventilation: In-hospital mortality was 55.9% in current nicotine dependence and 67.6% in never dependence.
- Short-term mortality: The adjusted risk ratios also stayed below 1.0 in these high-risk subgroup checks.
Year-by-year sensitivity analyses mostly pointed in the same direction from 2020 through 2023. The 2024 adjusted estimates were inconclusive, which the researchers attributed partly to fewer hospitalizations and lower mortality rates later in the pandemic.
The Result Needs a Narrow Reading
This result forces a careful distinction between association and causal advice. Nicotine dependence is harmful to health in many established ways, and this analysis does not overturn that.
It also does not separate nicotine itself from tobacco-smoke exposure, vaping, oral nicotine products, replacement therapy, or documentation practices.
The administrative dataset creates several boundaries:
- Coding uncertainty: ICD-10 nicotine-dependence codes were not externally validated for this study, so exposure misclassification is possible.
- Repeated admissions: The dataset tracked hospitalizations rather than unique people, so the same person could not be identified across admissions.
- Illness severity: The dataset lacked detailed COVID-19 severity, medication, and care-process information that could differ by nicotine-dependence status.
- Exposure detail: The analysis could not measure nicotine dose, product type, duration, or time since cessation.
- Generalizability: The records came from Texas hospitals, and the association may not transfer to other regions or future treatment periods.
The strongest reader-facing takeaway is not “nicotine protects against COVID-19.” A narrower statement fits the evidence: in a large Texas ICU administrative cohort, nicotine-dependence coding was associated with lower mortality even after measured adjustment, and the reason for the pattern remains uncertain.
The finding is a signal for follow-up research, especially studies that can measure smoking status, nicotine product, nicotine replacement therapy, disease severity, vaccination, antiviral treatment, admission timing, and care processes directly.
Citation: DOI: 10.1371/journal.pone.0308776. Garza et al. Nicotine dependence among critically ill COVID-19 patients: A population-based cohort study. PLOS One. 2026;21(4):e0308776.
Study Design: Population-based retrospective cohort study using Texas administrative inpatient records.
Sample Size: 142,045 adult ICU hospitalizations with principal-diagnosis COVID-19 from Q2 2020 through Q4 2024.
Key Statistic: Current nicotine dependence was associated with lower adjusted in-hospital mortality versus never dependence, with aRR 0.8955 and adjusted risk difference -0.0134.
Caveat: Administrative coding, residual confounding, repeated admissions, severity differences, and lack of nicotine-dose detail limit causal interpretation.





