TL;DR: A 2026 medRxiv preprint linked higher blood inflammatory markers with diffusion MRI signs of altered white-matter microstructure in 457 dementia-free middle-aged and older adults, especially for a combined cytokine score and orientation dispersion index.
Key Findings
- 457 dementia-free participants: The cross-sectional study examined adults with a mean age of 63.82 years and used blood markers plus diffusion MRI to test whether systemic inflammation tracked with white-matter microstructure.
- Cytokine composite showed the broadest pattern: A combined pro-inflammatory cytokine score was associated with higher cerebral free water fraction, orientation dispersion index, and mean diffusivity, with FDR-surviving coefficients for cerebral FWF, cerebral MD, and cerebellar ODI.
- CRP mainly tracked ODI: Higher high-sensitivity C-reactive protein was associated with higher orientation dispersion index in cerebral white matter and cerebellar peduncles, but these CRP links weakened after adding vascular-risk covariates.
- GFAP was less convincing globally: Glial fibrillary acidic protein, a blood marker related to astrocytic activation, did not show a significant global white-matter association after multiple-comparison correction.
- Alzheimer’s biomarkers did not explain the pattern: Results were broadly similar after accounting for the plasma Alzheimer’s pathology ratio p-tau181/A beta 42, although the authors noted that future samples with higher pathology are still needed.
Source: medRxiv (2026) | Mishra et al.
Blood Inflammation Was Compared With Diffusion MRI White-Matter Measures
White matter is the brain’s long-distance wiring system, and its microstructure can change with aging, vascular risk, inflammation, and neurodegenerative disease. The Mishra preprint asked whether blood markers of inflammation line up with diffusion MRI measures that are often used to probe white-matter tissue organization.
The study did not claim that a blood test can diagnose brain inflammation. It tested a narrower question: whether peripheral inflammation was associated with MRI-derived tissue metrics in people who were dementia-free at the time of assessment.
Researchers focused on three blood-marker groups:
- CRP: high-sensitivity C-reactive protein, a broad systemic inflammation marker often elevated in cardiometabolic and inflammatory states.
- Cytokine composite: a combined z-score across IL-1a, IL-1b, IL-2, IL-6, IL-8, TNF-a, and TNF-b, designed to capture a wider pro-inflammatory profile than any single cytokine.
- GFAP: glial fibrillary acidic protein, a blood marker linked to astrocyte injury or activation, though blood GFAP is not a direct image of brain inflammation.
The MRI side used diffusion measures: free water fraction (FWF), orientation dispersion index (ODI), and mean diffusivity (MD). These metrics describe how water moves through white-matter tissue and how dispersed the modeled fiber orientations are.
The 457-Person Sample Was Older but Not Dementia-Diagnosed
The analysis included 457 dementia-free adults. Mean age was 63.82 years, 68.7% were female, and the average Montreal Cognitive Assessment score was 26.31, a range consistent with generally intact cognition at the group level.
The paper was not studying advanced dementia. It looked for inflammation-linked tissue patterns in a late-middle-age and older-adult cohort where subtle brain-health differences can appear before a clinical diagnosis.
The sample also gave the study enough variation to compare several biological layers at once:
- Systemic inflammation: CRP and the cytokine composite captured peripheral inflammatory burden from blood.
- Astrocyte-related injury marker: GFAP tested whether a glial marker behaved like the systemic markers.
- Alzheimer’s pathology context: p-tau181/A beta 42 was included to see whether Alzheimer’s-related blood biomarker burden accounted for the white-matter associations.
- White-matter compartments: analyses separated broad cerebral white matter from cerebellar peduncle tracts.
Cytokines Had the Most Consistent White-Matter Association
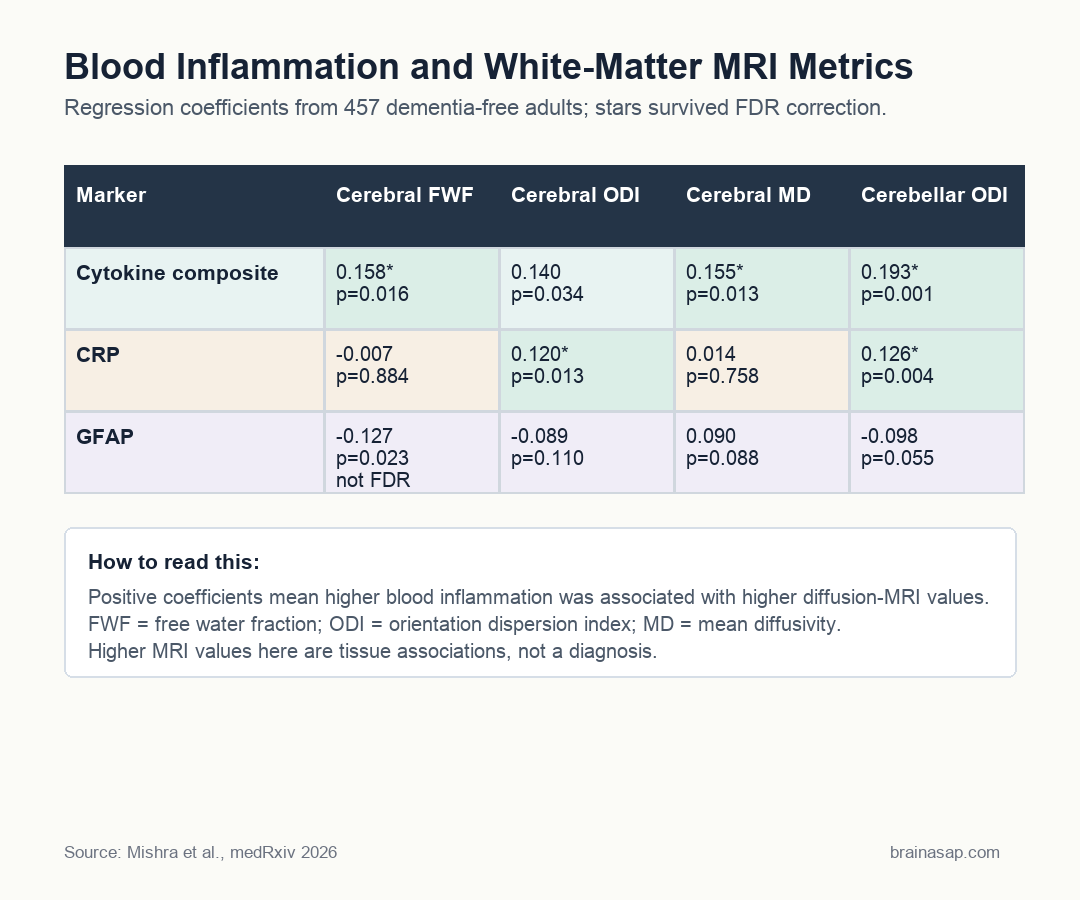
The clearest result was the cytokine composite. Higher cytokine scores were associated with higher cerebral FWF, higher cerebral ODI, and higher cerebral MD. The same marker also tracked with higher cerebellar ODI.
Several of those findings survived false-discovery-rate correction: cerebral FWF, cerebral MD, and cerebellar ODI. Cerebral ODI was significant before correction but was not marked as surviving the corrected threshold in the table.
The result fits the researchers’ interpretation that diffusion MRI may be sensitive to inflammatory processes, especially when inflammation is represented as a broader cytokine profile rather than a single molecule.
It also keeps the claim bounded: these are associations, not proof that the cytokines caused white-matter change.
CRP Tracked Orientation Dispersion, but Vascular Risk Complicated It
CRP showed a narrower association. Higher CRP was associated with higher ODI in both cerebral white matter and cerebellar peduncles, with p values of 0.013 and 0.004, respectively.
The sensitivity analysis made that result more cautious. When researchers added body mass index and a vascular-risk summary score, the CRP associations were no longer significant.
- Primary model: CRP tracked higher ODI in both cerebral white matter and cerebellar peduncles.
- Vascular-risk model: the CRP associations weakened after adding body mass index and vascular-risk burden.
- Interpretation: CRP likely reflects systemic vascular-metabolic inflammation more than a clean brain-specific marker.
That does not make the CRP result useless, but it does suggest the CRP-white-matter link may overlap with vascular and metabolic health rather than reflecting a clean brain-specific inflammation marker.
The paper’s more stable message is therefore not “CRP identifies brain inflammation.” A better reading is that broad systemic inflammation, vascular risk, and white-matter microstructure are entangled in aging samples.
GFAP and Alzheimer’s Biomarkers Did Not Explain the Cytokine Pattern
GFAP was the marker that most clearly diverged from the others. It showed an uncorrected association with lower cerebral FWF, but that result did not remain significant after correcting for multiple comparisons.
That distinction is important because GFAP is often discussed as a brain-relevant blood biomarker. In this global white-matter analysis, it did not produce the same robust pattern as the cytokine composite.
The study leaves two possible interpretations open:
- Global metrics were broad: GFAP could relate to specific tracts or regional injury patterns that disappear when white matter is averaged into large composites.
- Peripheral markers differ biologically: cytokines and CRP may capture systemic inflammatory burden, while GFAP may reflect a different glial or injury-related process.
- Blood is not brain tissue: plasma GFAP and cytokines are indirect measures, so cerebrospinal fluid or more region-specific imaging could produce a different picture.
Researchers also adjusted for p-tau181/A beta 42, a blood ratio related to Alzheimer’s disease pathology. The main inflammatory-marker findings were broadly consistent after that adjustment.
That adjustment narrows the interpretation. The white-matter associations were not simply explained away by the Alzheimer’s biomarker ratio in this dementia-free sample.
Future cohorts with higher Alzheimer’s pathology are still needed to test whether inflammation and pathology interact more strongly in higher-risk groups. This is not a new screening test; it is evidence that blood inflammation and diffusion MRI white-matter measures may carry overlapping information about brain aging.
Cross-Sectional Design Keeps the Claim Cautious
The main limitation is straightforward: this was a cross-sectional observational study. Blood markers and MRI were measured in relation to each other, but the design cannot show which came first or whether lowering inflammation would change white-matter microstructure.
Other limits also keep the interpretation narrow:
- Peripheral inflammation is indirect: blood cytokines and CRP do not prove neuroinflammation inside the brain.
- Regional patterns may be missed: global cerebral and cerebellar composites can hide tract-specific effects.
- Preprint status: the manuscript was posted to medRxiv and had not been peer reviewed at the time of posting.
Still, the study gives a concrete result: in dementia-free older adults, a broader cytokine score lined up with several diffusion MRI measures of white-matter microstructure.
That is a useful bridge between blood-based aging biology and non-invasive brain imaging, provided the finding is treated as an association that needs longitudinal confirmation.
Citation: DOI: 10.64898/2026.04.20.26351124. Mishra et al. Plasma inflammatory markers and brain white matter microstructure in late middle-aged and older adults. medRxiv. 2026.
Study Design: Cross-sectional observational analysis of blood inflammatory markers and diffusion MRI white-matter metrics.
Sample Size: 457 dementia-free middle-aged and older adults; mean age 63.82 years.
Key Statistic: Cytokine composite associations survived FDR correction for cerebral FWF, cerebral MD, and cerebellar ODI; CRP associations survived for cerebral and cerebellar ODI in the primary model.
Caveat: Blood inflammation, MRI microstructure, and vascular risk were measured at one time point, so the study cannot establish causality or diagnostic use.





