TL;DR: A 2026 randomized pilot trial in the Journal of Affective Disorders found that 30 minutes of moderate exercise before cognitive behavioral therapy (CBT) for major depressive disorder was linked to stronger therapy-process measures and higher exploratory remission than quiet rest before CBT.
Key Findings
- Forty adults with major depressive disorder were randomized: Nineteen received exercise before CBT, and 21 received a quiet, time-matched control period before CBT.
- Exercise priming meant 30 minutes of moderate activity: Participants exercised immediately before each weekly therapy session for 8 weeks.
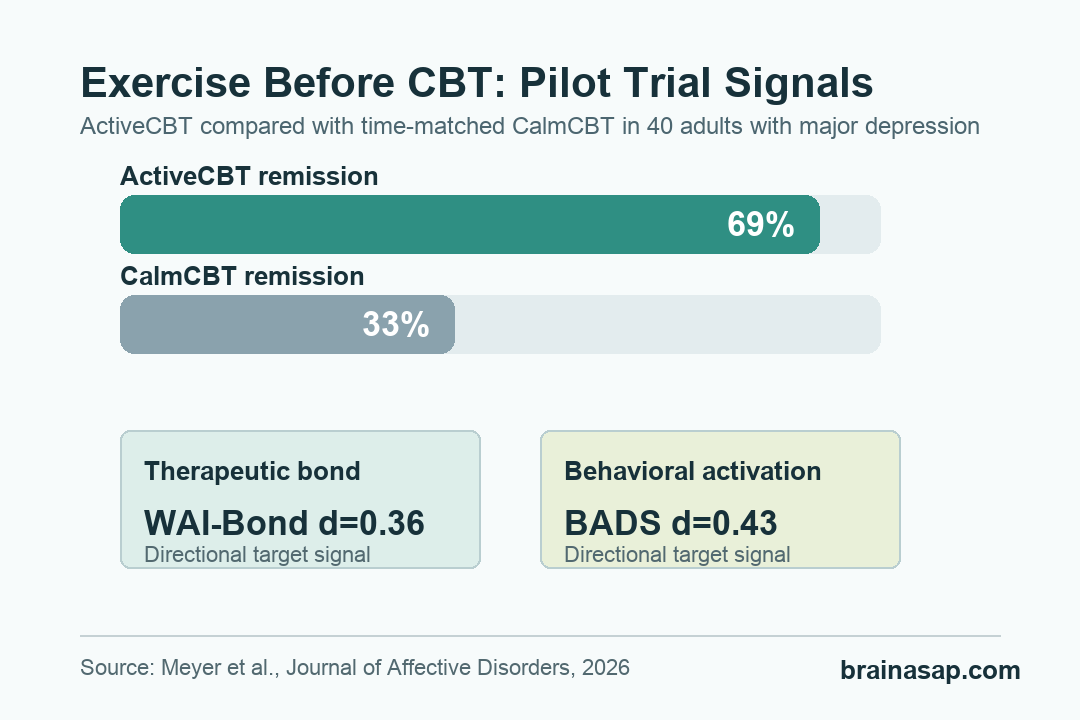
- Therapeutic bond favored exercise: The Working Alliance Inventory bond subscale showed a standardized effect of d=0.36 for ActiveCBT.
- Behavioral activation also favored exercise: Behavioral Activation for Depression Scale change showed d=0.43, a directional target-engagement result.
- Remission was higher in exploratory analysis: Hamilton depression remission was 69% with exercise before CBT versus 33% with quiet rest before CBT.
Source: Meyer et al. Journal of Affective Disorders. 2026.
A therapy session begins with the patient’s current mood state, energy level, stress level, and readiness to act.
This trial tested whether a short bout of moderate exercise could change that pre-session state enough to strengthen CBT for depression.
The comparison was practical. One group did 30 minutes of individual moderate exercise immediately before each CBT session.
The other group spent the same amount of time in a calm, attention-matched control condition before therapy.
Researchers called the exercise condition ActiveCBT and the control condition CalmCBT. Both groups then received the same standardized CBT program.
The key question was not whether CBT works. It was whether the minutes before therapy could help therapy work better.
Exercise Before CBT Targeted Two Therapy Mechanisms
The trial focused on mechanisms rather than a definitive treatment effect. The two primary targets were therapeutic alliance and behavioral activation.
Therapeutic alliance was measured with the Working Alliance Inventory-Short Revised, a questionnaire about the patient-therapist relationship. The researchers looked at total alliance and three subdomains:
- Bond: The sense of trust, emotional connection, and being understood by the therapist.
- Tasks: Agreement about what the patient and therapist are doing during treatment.
- Goals: Agreement about what therapy is trying to accomplish.
Behavioral activation was measured with the Behavioral Activation for Depression Scale (BADS), which tracks engagement with rewarding or meaningful activities. CBT often works partly by helping people move from avoidance and withdrawal toward action.
The researchers set a progression rule before the study: exercise priming would look promising if it produced a standardized effect of at least d=0.35 on both mechanism targets, or d=0.55 on either one.
ActiveCBT Showed Directional Gains in Therapy Bond
The strongest alliance difference was not in the total Working Alliance score. It came from the bond subscale, where ActiveCBT showed a standardized effect of d=0.36.
That distinction is important. A stronger emotional bond with the therapist is different from simply agreeing on homework or treatment goals.
The researchers noted that acute exercise could plausibly affect mood, stress reactivity, social engagement, and readiness for interpersonal connection.
Behavioral activation moved in the same direction. BADS change favored ActiveCBT with a standardized effect of d=0.43, and the average between-group effect was 7.78 points, although the confidence interval crossed zero and the p value was 0.093.
Taken together, the two mechanism results met the trial’s pre-specified progression rule. Exercise before therapy is still not proven as a depression treatment.
It means the pilot found enough target engagement to justify a larger trial.
Remission Was Higher After Exercise-Primed Therapy
Depression outcomes were secondary and exploratory. The study was too small to serve as a final efficacy test.
Still, the remission difference was clinically relevant.
Remission was defined as a Hamilton Rating Scale for Depression (HAMD) score below 8, assessed by a masked interviewer. After treatment, 69% of ActiveCBT participants met remission criteria compared with 33% of CalmCBT participants.
Response rates were more similar between groups, meaning the clearer exploratory separation was remission rather than a 50% symptom reduction threshold.
In practical terms, the exercise group showed more than a small average symptom edge; more participants crossed into a low-symptom range.
The trial also reported good adherence. Across both groups, participants attended 281 of 320 planned visits, or 87.8%. Thirty-three of 40 participants completed all 8 sessions, and 34 completed at least 6 sessions.
The Control Condition Was More Than No Treatment
A useful feature of this study is that CalmCBT was not a waitlist or usual-care comparison. It matched the exercise group for time and attention before therapy, which makes the exercise-specific question cleaner.
The intervention check also showed that the two pre-therapy periods were physically different. ActiveCBT participants had higher exertion ratings and higher heart rates during the pre-therapy period:
- Exercise intensity: ActiveCBT participants reported an average perceived exertion of 13.0.
- Control intensity: CalmCBT participants reported an average perceived exertion of 6.22.
- Heart rate: ActiveCBT averaged 124.0 beats per minute, compared with 74.9 beats per minute in CalmCBT.
CBT fidelity was similar between groups, which reduces the chance that the difference was simply caused by one group receiving better therapy.
The researchers also reported no unanticipated adverse events, and no participants reported an intervention-related adverse event at post-treatment.
The Main Limitation Is Sample Size
The evidence should be read as preliminary. The trial randomized 40 adults, and it was designed to test target engagement, not to prove clinical efficacy. Confidence intervals for the mechanism outcomes included zero.
There was also no long-term follow-up in the published report, so the study cannot show whether remission lasted or whether relapse rates changed. The sample also excluded some people for safety or clinical reasons, including people unable to safely participate in physical activity.
Those limits define the evidence. In this small randomized trial, exercise immediately before CBT produced directional gains in two therapy mechanisms and a higher exploratory remission rate.
For now, the trial is best understood as a testable augmentation idea: a brief, structured exercise session may help some people arrive at therapy more ready to connect, plan, and act.
Citation: DOI: 10.1016/j.jad.2026.121606. Meyer et al. Exercise priming to enhance therapeutic bond and behavioral activation in CBT for MDD: a randomized controlled target-engagement trial with remission signal. Journal of Affective Disorders. 2026;405:121606.
Study Design: Severity-stratified randomized controlled target-engagement trial comparing exercise before CBT with a time- and attention-matched calm control before CBT.
Sample Size: Forty adults with DSM-5 major depressive disorder; 19 assigned to ActiveCBT and 21 assigned to CalmCBT.
Key Statistic: HAMD remission was 69% with exercise before CBT versus 33% with calm control before CBT; WAI-Bond d=0.36 and BADS d=0.43 favored ActiveCBT.
Caveat: This was a small pilot trial designed for mechanism measures, not a definitive efficacy trial, and longer-term durability was not tested.