TL;DR: A 2026 study in European Journal of Psychotraumatology found that 3 days of Community Resiliency Model (CRM) training, a body-based trauma-regulation skills program, improved compassion, social cohesion, forgiveness, and resilience among 152 Rwandan genocide survivors, released perpetrators, and mixed survivor-perpetrator groups.
Key Findings
- Three groups completed CRM training: Researchers studied 51 genocide survivors, 51 released perpetrators, and 50 mixed-group participants in rural Rwanda.
- Compassion showed the largest statistical change: Compassion improved over time with F = 131.60 and partial eta squared of 0.48.
- Social cohesion also increased: Social-cohesion scores improved with F = 36.19 and partial eta squared of 0.20.
- Forgiveness and resilience improved too: Forgiveness and resilience both increased from baseline, though resilience had the smallest effect size.
- Mixed groups were not worse: Improvements did not significantly differ between survivor-only, perpetrator-only, and mixed survivor-perpetrator groups.
Source: The paper appeared in European Journal of Psychotraumatology and studied a community trauma-recovery intervention in Rwanda, not a medication or individual psychotherapy trial.
Community recovery after mass violence is not only about symptom reduction. Trust, forgiveness, compassion, and social cohesion can remain damaged long after formal conflict ends.
This study tested whether Community Resiliency Model (CRM) training could shift those social-function outcomes in Rwandan communities affected by the 1994 genocide against the Tutsi.
3 Days of CRM Training Were Tested in 152 Adults
The researchers used a longitudinal randomized comparison design with three participant groups. One group included genocide survivors, one included released genocide perpetrators, and one mixed both groups together.
All participants completed 3 consecutive days of CRM skills training in community settings. Outcomes were measured at baseline, immediately after the intervention, and again at 6 months.
- Survivor-only group: 51 people who survived the genocide.
- Perpetrator-only group: 51 released genocide perpetrators living in the community.
- Mixed group: 50 people trained together across survivor and perpetrator status.
The outcomes were deliberately social rather than narrowly clinical. Researchers measured resilience, compassion, social cohesion, and forgiveness using standardized scales translated into Kinyarwanda.
The intervention was aimed at community repair. A treatment that lowers distress but leaves mistrust unchanged would not answer the same public-health problem.
Compassion and Social Cohesion Had the Strongest Gains
Across all groups, repeated-measures analysis showed statistically significant improvements in the 4 social-function outcomes. Compassion had the largest effect, with F = 131.60, p < .001, and partial eta squared of 0.48.
Social cohesion also improved substantially, with F = 36.19, p < .001, and partial eta squared of 0.20. Forgiveness improved as well, with F = 19.87, p < .001, and partial eta squared of 0.12.
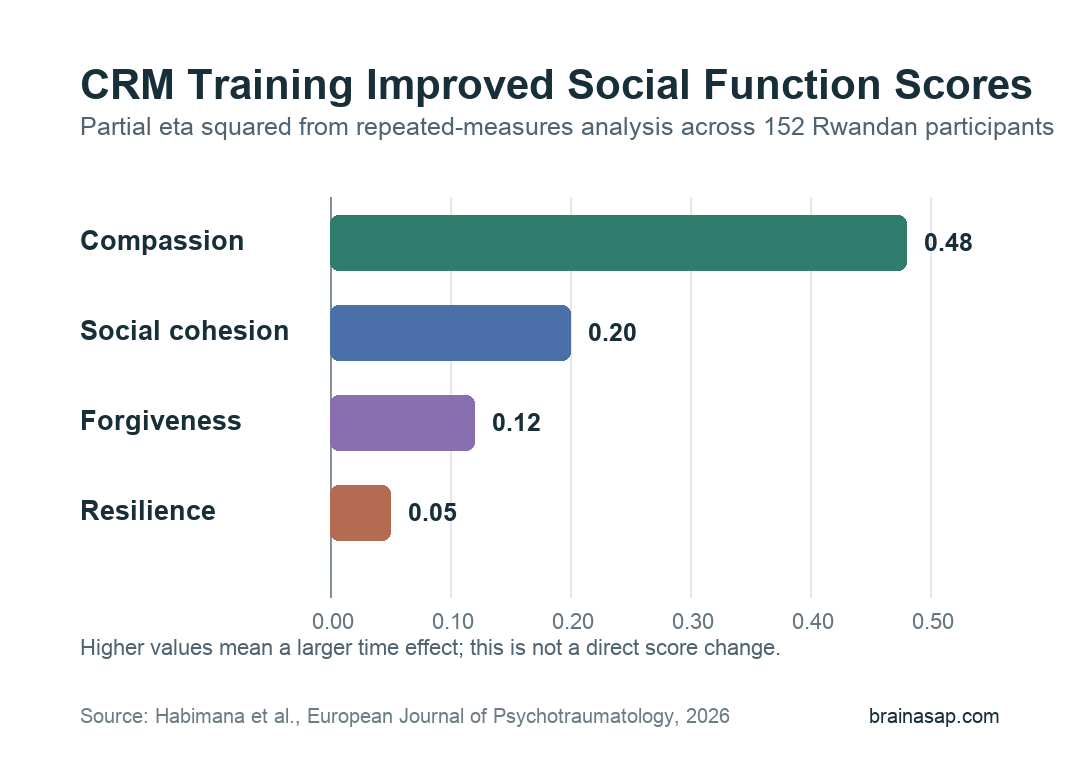
Resilience improved too, but the effect size was smaller: F = 8.10, p = .005, and partial eta squared of 0.05. The paper reports this as a significant but more modest change.
- Compassion: Large time effect across the follow-up period.
- Social cohesion: Clear improvement in community-relationship functioning.
- Forgiveness: Statistically significant improvement across groups.
- Resilience: Significant but smaller improvement than the relational outcomes.
The pattern suggests that CRM may have been strongest where the target was relational stance and social functioning, not only individual coping capacity.
Mixed Survivor-Perpetrator Groups Were Not Inferior
A central design issue was whether mixed survivor-perpetrator training would perform worse, better, or similarly to separate groups. The study did not find significant differences in improvement between the three delivery formats.
The delivery-format result has practical value because mixed community life is often unavoidable after conflict. If mixed groups were harmful or clearly less effective, community programs would need a different structure.
Instead, the mixed group showed gains that were broadly comparable to the survivor-only and perpetrator-only groups. Compassion in the mixed group increased from 20.82 at baseline to 29.86 at 6 months.
Social cohesion in the mixed group increased from 59.00 at baseline to 74.36 immediately after training, then stabilized at 67.74 at 6 months.
- Not a superiority finding: The mixed group was not statistically better than the other groups.
- Not an inferiority finding: Mixed training did not show worse improvement than separate survivor-only or perpetrator-only training.
- Practical implication: Carefully facilitated mixed groups may be feasible when communities already require daily coexistence.
The paper frames mixed and homogeneous formats as complementary rather than one universal model. That is a reasonable boundary for a small community study.
CRM Focused on Body-Based Regulation Skills
CRM is not exposure therapy and not a reconciliation lecture. The intervention teaches body-based skills intended to help people notice stress responses, return to the present, and access sources of stability.
The six skills included tracking, resourcing, grounding, gesturing, Help Now, and Shift and Stay. In the Rwandan implementation, training was delivered in Kinyarwanda by local CRM teachers, psychotherapists, and social workers.
- Tracking: Noticing body sensations and how they connect with stress or stability.
- Resourcing: Identifying people, memories, beliefs, or experiences linked with comfort or strength.
- Grounding: Using present-moment contact with the body and environment to reduce overwhelm.
- Shift and Stay: Moving attention from distress toward neutral or positive sensations long enough to regain balance.
The mechanism proposed by the researchers is straightforward: better regulation may make compassion, forgiveness, and social contact easier to sustain. The study did not prove the mechanism directly, but the outcome pattern fits that interpretation.
The Evidence Is Promising but Not Definitive
The strongest feature is the follow-up design. Participants were assessed immediately after training and again at 6 months, so the paper did not rely only on short-term post-session enthusiasm.
Several limits keep the conclusion cautious. The sample was 152 participants, recruitment used a convenience sample, and the study did not include a no-treatment control group.
Researchers also note that follow-up occurred near Rwanda’s national genocide commemoration period, when stress and trauma symptoms can increase. That timing could have affected six-month scores.
- No untreated control group: The design cannot fully separate CRM effects from time, repeated measurement, or outside community factors.
- Single rural district: Results may not generalize to urban settings or other post-conflict contexts.
- Quantitative-only evaluation: The study did not include qualitative interviews that could explain how participants experienced the mixed-group format.
The practical takeaway is that CRM training was associated with better social-function scores in a difficult post-genocide setting.
For policy or clinical use, the next step would be a larger randomized controlled trial with a comparison condition, broader districts, and qualitative data on safety, trust, and group dynamics.
Citation: DOI: 10.1080/20008066.2026.2621634. Habimana et al. Promoting social cohesion, compassion and forgiveness among Rwandan survivors and perpetrators through community resiliency model training: a longitudinal randomized comparison study. European Journal of Psychotraumatology. 2026;17:2621634.
Study Design: Longitudinal randomized comparison study of CRM training across survivor-only, perpetrator-only, and mixed survivor-perpetrator groups.
Sample Size: 152 adults in rural Rwanda, including 51 survivors, 51 released perpetrators, and 50 mixed-group participants.
Key Statistic: Compassion improved with F = 131.60, p < .001, and partial eta squared of 0.48; social cohesion improved with F = 36.19, p < .001, and partial eta squared of 0.20.
Caveat: The study used a small convenience sample, lacked a no-treatment control group, and was conducted in one rural district.