TL;DR: A pilot cohort study in JMIR Rehabilitation and Assistive Technologies found that online emotional training after facial palsy surgery improved facial movement, social well-being, and anxiety about as much as in-person therapy in 16 adults.
Key Findings
- Population: The study followed 16 adults after triple innervation surgery for unilateral peripheral facial nerve palsy.
- Delivery: 8 participants trained in person, while 8 completed the same emotional training protocol by telerehabilitation.
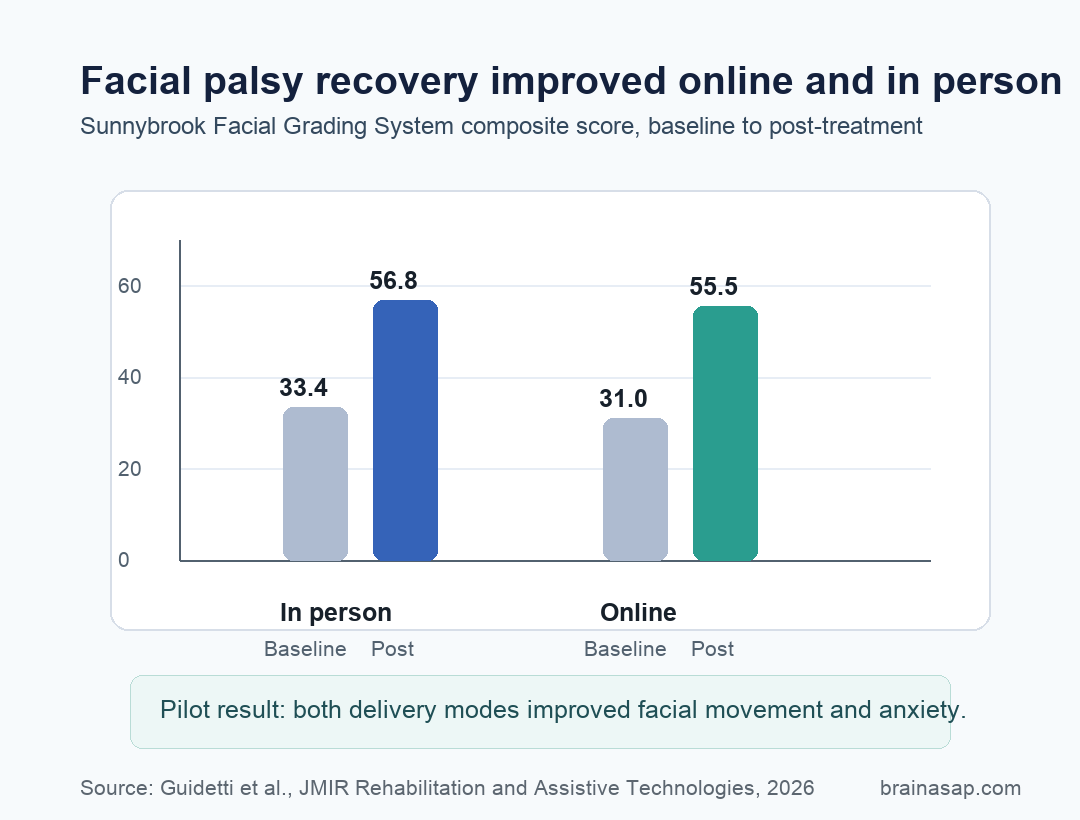
- Facial movement: Sunnybrook Facial Grading System composite scores improved from 33.4 to 56.8 in person and from 31.0 to 55.5 online.
- Anxiety: Beck Anxiety Inventory scores fell from 20.13 to 13.12 in person and from 13.5 to 9.75 online.
- Main caveat: The pilot was small, nonrandomized, and had no long-term follow-up, so it supports feasibility more than definitive efficacy.
Source: Guidetti et al. 2026.
Facial nerve palsy is not only a problem of weak muscles. When one side of the face cannot smile, blink, or move normally, patients can lose facial symmetry, daily function, and social confidence at the same time.
That is why this study tested a rehabilitation approach that treated facial movement as both a motor task and an emotional-expression task.
Researchers studied emotional training, a protocol that combines sensory attention, motor control, emotional expression practice, and functional facial exercises. The study question was practical: after triple innervation surgery, could patients do this training online without losing the gains expected from in-person care?
Online Emotional Training Matched In-Person Facial Palsy Therapy
The study included 16 adults with unilateral peripheral facial nerve palsy who had undergone triple innervation surgery. Participants received a 45- to 50-minute session every 2 weeks for 20 weeks, for a total of 10 sessions.
Assignment was based on whether patients could attend in person, not randomization. That means the study cannot prove that online therapy is equivalent in the strict trial sense.
Still, the comparison was clinically useful because both groups received the same emotional training framework, delivered through different routes.
The protocol targeted three connected goals:
- Selective facial control: Patients practiced activating facial muscles more precisely after nerve transfer surgery.
- Emotional expression: Training worked on spontaneous and emotionally congruent expressions, not only isolated facial movements.
- Daily function: Later exercises connected movement practice to eating, speaking, smiling, and social communication.
Sunnybrook Facial Scores Improved in Both Groups
The main motor scale was the Sunnybrook Facial Grading System, or SFGS, which rates facial resting symmetry, voluntary movement, synkinesis, and an overall composite score. Higher composite scores indicate better facial function.
Both groups improved substantially. The in-person group moved from a mean SFGS composite score of 33.4 at baseline to 56.8 after treatment.
The online group moved from 31.0 to 55.5. The time effect was significant at P < .001, and the treatment-delivery difference was not significant.
Voluntary movement improved in the same direction. SFGS symmetry of voluntary movement increased from 46.0 to 63.0 in the in-person group and from 45.5 to 63.0 online.
With bilateral masseter contraction, composite scores also rose in both groups, from 48.5 to 65.9 in person and from 46.1 to 67.9 online.
Anxiety and Social Well-Being Also Moved in the Right Direction
The emotional part of the intervention matters because facial palsy can make social interaction exposed and effortful. A face that does not move symmetrically can change how people smile, eat in public, speak, and read emotional feedback from others.
Across both groups, the Facial Disability Index social and well-being score improved, with a significant time effect at P < .001. Anxiety also improved.
Beck Anxiety Inventory scores declined from 20.13 to 13.12 in the in-person group and from 13.5 to 9.75 online, with a significant time effect at P = .002.
The only outcome where delivery route clearly differed was the Facial Disability Index physical function subscale. The in-person group improved more on that measure, with a time-by-treatment interaction of F1 = 14.356; P = .002.
That does not erase the online gains, but it does suggest that some physical-function elements may still benefit from direct hands-on care.
The Rehabilitation Target Was Facial Expression, Not Just Strength
Triple innervation surgery uses several neural inputs to restore facial movement. In this study, rehabilitation had to help patients coordinate those new inputs into usable expression.
That is a harder task than simply asking a muscle to contract.
Emotional training tries to rebuild expression through sensory-motor and emotional pathways. The paper describes a progression from recognizing sensations on the affected side of the face, to practicing voluntary movement, to restoring expressive gestures in real-life tasks.
That structure makes the online result important. If a trained therapist can guide enough of that process remotely, telerehabilitation may help patients who face:
- Travel barriers: specialized facial palsy rehabilitation may be available only at distant centers.
- Social discomfort: some patients may avoid frequent public appointments because of facial asymmetry.
- Continuity problems: a home-based option may keep therapy going when in-person attendance is difficult.
The Pilot Design Keeps the Result Preliminary
The strongest interpretation is feasibility, not proof of equivalence. The study had 16 participants, no random assignment, and no follow-up showing whether gains lasted after the 20-week program ended.
Participants also had different causes of facial palsy, including neurinoma, trauma, and surgical causes.
Medication details were not documented, and the neurophysiological explanation was not tested with imaging. Those limits matter because motor recovery after facial reanimation can vary by surgical timing, cause of palsy, baseline impairment, and treatment adherence.
Still, adherence was notable: the paper reported no dropouts in either group. For a small postoperative rehabilitation study, that supports the idea that online emotional training is acceptable enough to test in larger, more rigorous trials.
Remote Facial Palsy Rehab Needs a Larger Trial Next
Online emotional training appeared feasible and produced motor, social, and anxiety improvements similar to in-person delivery on most measured outcomes in this small cohort.
For patients, this should not be read as proof that remote therapy can replace all hands-on facial palsy rehabilitation. For clinicians, it points to a testable model: keep the structured emotional-training protocol, measure facial motor recovery and psychosocial outcomes, and run a larger randomized trial with longer follow-up.
Citation: DOI: 10.2196/79520. Guidetti et al. Emotional Training via Telerehabilitation After Surgical Treatment for Facial Palsy: Prospective, Assessor-Blinded, 2-Arm Pilot Cohort Study. JMIR Rehabilitation and Assistive Technologies. 2026;13:e79520.
Study Design: Prospective, assessor-blinded, 2-arm pilot cohort study comparing in-person and online emotional training.
Sample Size: 16 adults after triple innervation surgery for unilateral peripheral facial nerve palsy.
Key Statistic: SFGS composite scores improved from 33.4 to 56.8 in person and from 31.0 to 55.5 online, with a significant time effect at P < .001.
Caveat: Small nonrandomized pilot study without long-term follow-up, so the findings are hypothesis-generating.