TL;DR: A 2026 HomePAP secondary analysis in Journal of Clinical Sleep Medicine found that higher PAP mask leak predicted lower obstructive sleep apnea treatment adherence, but a new Real Leak measure, unintentional leak after subtracting expected mask leak, did not outperform conventional Average Leak.
Key Findings
- HomePAP sample size: PAP data were available for 139 HomePAP participants at 1 month and 124 at 3 months.
- 46.2% adherence at 3 months: By 3 months, 61 of 132 measured participants met the common 4-hours-on-70%-of-nights adherence rule.
- Real Leak tracked Average Leak: Real Leak and Average Leak were highly correlated at 1 month (rho 0.73) and 3 months (rho 0.90).
- Higher leak predicted lower use: Each 1 L/min increase in Real Leak corresponded to 2.66 fewer minutes of average daily PAP use, and a 10 L/min difference corresponded to a 7.2-point drop in 4-hour-use days.
- No clear metric winner: Real Leak and Average Leak predicted adherence similarly, so the main value is clearer terminology rather than better prediction.
Source: Journal of Clinical Sleep Medicine (2026) | Andrews et al.
PAP Mask Leak Predicted Sleep Apnea Treatment Adherence
Positive airway pressure (PAP) therapy can work well for obstructive sleep apnea, but only when people use it enough. Mask leak is one common reason PAP feels uncomfortable, noisy, dry, or ineffective.
This study tested whether a clearer leak measure better explained adherence. The proposed metric was called Real Leak, meaning unintentional leak after subtracting the expected intentional leak built into a specific mask at a specific pressure.
The clinical problem is practical. PAP machines can report several leak values, and clinicians do not always know which value best identifies a mask-fit problem that will reduce nightly use.
Real Leak Subtracted Expected Mask Leak From Average Leak
All PAP masks are designed to vent some air intentionally. That intentional leak helps clear carbon dioxide from the mask and is not the same as unwanted air escaping from a poor seal.
Researchers calculated Real Leak by starting with device-reported Average Leak and subtracting mask-specific intentional leak. In plain terms, Real Leak was meant to approximate unintentional leak over the prior month.
The comparison metric was Average Leak, a familiar value recorded by PAP devices across the usage period. Researchers asked whether Real Leak would be more strongly associated with adherence than Average Leak.
- Average Leak: Total average leak reported by the PAP device during the recording period.
- Intentional leak: Expected mask venting needed at a given pressure for safe ventilation.
- Real Leak: Average Leak minus expected intentional leak, intended to isolate unwanted leak.
- Adherence rule: PAP use for at least 4 hours per night on at least 70% of nights.
This distinction is clinically clear even if the numbers remain highly related. A patient cannot fix intentional venting, but clinicians can often adjust mask size, mask type, cushion fit, pressure comfort, humidity, or coaching when unintentional leak is high.
HomePAP Data Included 139 Participants at 1 Month
The analysis used data from the HomePAP trial, which randomized adults at high risk for obstructive sleep apnea to home sleep apnea testing or laboratory polysomnography, followed by PAP initiation.
Participants had moderate-to-severe obstructive sleep apnea risk. The median apnea-hypopnea index (AHI), the number of breathing interruptions per hour of sleep, was 36.8, which falls in the severe range.
Data were available for 139 participants at 1 month and 124 participants at 3 months. The full baseline sample had a mean age of 48.4 years, 65.3% male participants, and median body mass index of 36.3 kg/m2.
PAP adherence was modest. At 1 month, 36.9% met the 4-and-70 adherence criterion. At 3 months, adherence increased to 46.2%, with average days of at least 4 hours of use reaching 63.3%.
Real Leak and Average Leak Were Highly Correlated
Real Leak and Average Leak moved together. The correlation was rho 0.73 at 1 month and rho 0.90 at 3 months, with p < 0.001 at both timepoints.
That strong correlation is expected because Real Leak is calculated from Average Leak. Subtracting intentional leak changes the meaning of the value, but it does not create a fully independent measurement.
Median 3-month Real Leak was 15.5 L/min, while median 3-month Average Leak was 41.4 L/min. The gap reflects the intentional leak built into PAP masks and pressure settings.
Both leak measures predicted lower adherence after adjustment for age, sex, body mass index, race, education, baseline Epworth Sleepiness Scale score, and AHI. The result supports the general clinical point that leak and adherence are linked.
Each 10 L/min Real Leak Increase Predicted 7.2% Fewer Adherent Days
The regression results gave the leak finding a practical size. Each 1 L/min increase in Real Leak corresponded to a 2.66-minute decrease in average daily PAP use.
The same 1 L/min Real Leak increase corresponded to a 0.72 percentage-point decrease in days with at least 4 hours of PAP use. Scaling that to 10 L/min gives a 26.6-minute drop in average daily PAP use and a 7.2 percentage-point decrease in adherent days.
Average Leak showed a similar but slightly smaller association. Each 1 L/min increase corresponded to 2.01 fewer minutes of average daily use and 0.55 percentage-point fewer days with at least 4 hours of use.
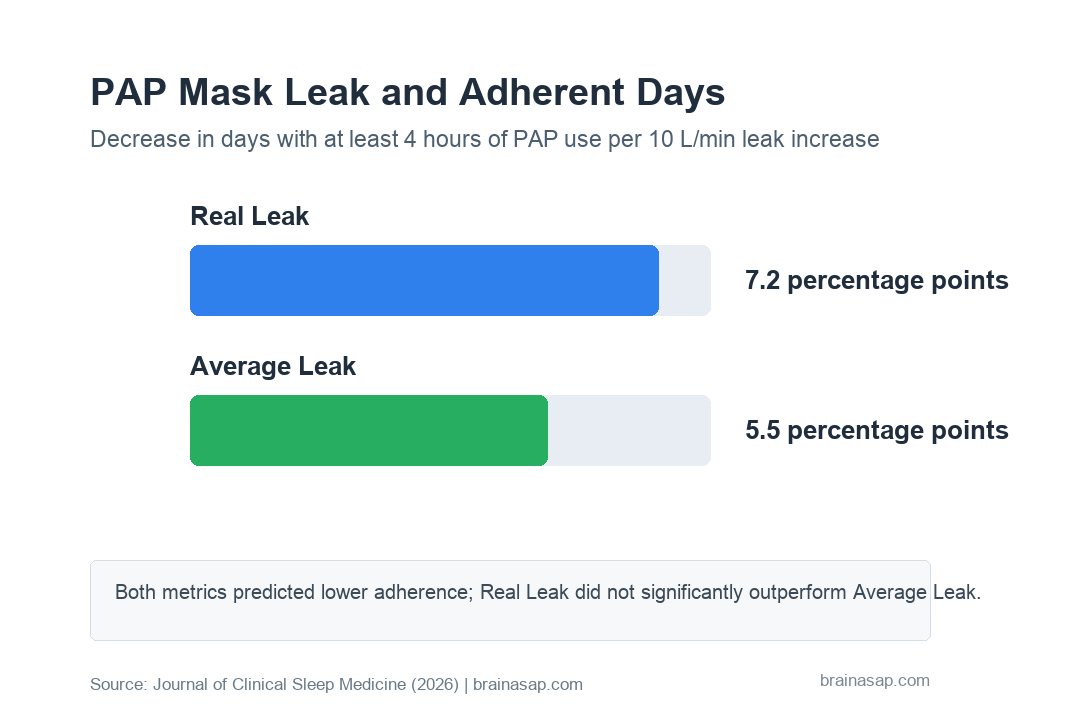
- Real Leak per 10 L/min: 26.6 fewer minutes of average daily PAP use and 7.2 percentage points fewer adherent days.
- Average Leak per 10 L/min: 20.1 fewer minutes of average daily PAP use and 5.5 percentage points fewer adherent days.
- Performance comparison: The study did not find a significant predictive advantage for Real Leak over Average Leak.
Race and AHI were also independent adherence predictors.
White race was associated with a higher percentage of adherent days than Black race, and higher AHI was associated with greater adherence. Those findings point to social, clinical, and symptom-severity factors beyond leak alone.
Leak terminology matters more than a new score:
The main outcome was not that Real Leak replaces Average Leak. Instead, both measures were negatively associated with adherence, and neither clearly outperformed the other.
Real Leak can still help by giving clinicians a cleaner label for the problem they are trying to fix.
Average Leak mixes expected mask venting with unwanted leak; Real Leak tries to isolate the unwanted component.
Inconsistent PAP leak reporting can weaken clinical follow-up. Devices, studies, and clinical workflows can refer to average leak, large leak, time in leak, expected leak, or unintentional leak without using the same definitions.
For a patient, the practical question is not which variable sounds more technical. The question is whether a leak value prompts concrete troubleshooting before frustration turns into nonadherence.
Real Leak Needs Longer and More Device-Diverse Testing
The study has several limits. Follow-up lasted only 3 months, so long-term adherence is unknown.
All participants used one device platform, Respironics REMstar Auto. Leak definitions and device algorithms can differ across manufacturers, which limits generalization.
The HomePAP trial also involved academic sleep centers, where education, titration, mask access, and follow-up can differ from everyday sleep-clinic practice. Real-world adherence can be shaped by insurance rules, supply replacement, coaching access, and patient cost.
- Shared information: Real Leak is derived from Average Leak, so similar predictive performance is expected.
- Averaged data: 30-day leak averages can hide night-to-night or within-night leak bursts that affect comfort.
- No clear cut-point: The study supports leak as an adherence marker but does not define a universal Real Leak threshold for intervention.
- Broader adherence barriers: Education time, troubleshooting interventions, and PAP optimism did not predict adherence here, but unmeasured comfort, access, and support factors can still matter.
The actionable result is straightforward: clinicians should keep mask leak visible when reviewing PAP downloads, but they should not assume one adjusted leak score solves adherence management. Clear leak definitions, compatible masks and devices, and early troubleshooting remain the main clinical targets.
Citation: DOI: 10.1007/s44470-026-00046-2. Andrews et al. What’s leak got to do with it? Association of mask leak and positive airway pressure adherence from the HomePAP study. Journal of Clinical Sleep Medicine. 2026;22:55.
Study Design: Secondary analysis of HomePAP trial data comparing Real Leak and Average Leak associations with PAP adherence.
Sample Size: 139 participants with 1-month PAP data and 124 participants with 3-month PAP data.
Key Statistic: Each 10 L/min increase in Real Leak corresponded to 26.6 fewer minutes of average daily PAP use and 7.2 percentage points fewer adherent days.
Caveat: 3-month follow-up, one PAP device platform, academic sleep-center sample, and Real Leak was mathematically derived from Average Leak.





