TL;DR: A 2026 review in Neuroscience & Biobehavioral Reviews found that chronic primary pain studies most consistently linked higher pain sensitivity with lower mean arterial pressure, higher cortisol, higher heart rate during recovery, and lower parasympathetic recovery.
Key Findings
- The evidence base covered 52 studies; 37 contributed qualitative evidence and 21 had enough data for meta-analysis.
- The analyzed chronic pain sample totaled 1,137 participants, including 653 people with chronic widespread pain and 484 with chronic localized pain.
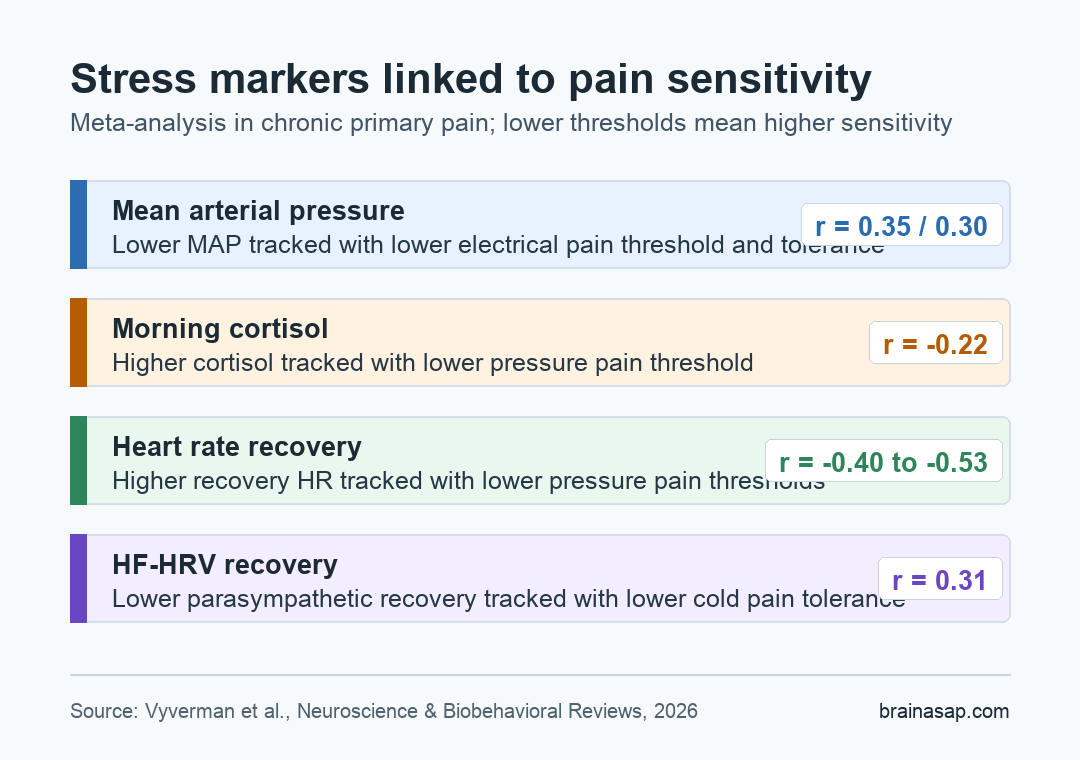
- Lower mean arterial pressure was associated with lower electrical pain threshold and tolerance, a pattern consistent with weaker blood-pressure-related pain modulation.
- Higher baseline cortisol was associated with lower pressure pain threshold, suggesting a possible HPA-axis link to heightened sensitivity.
- Higher heart rate during recovery and lower high-frequency heart-rate variability during recovery were consistent with slower autonomic settling after stress.
Chronic primary pain is often described as a pain problem. The physiology around pain also includes stress-response systems that adjust heart rate, blood pressure, and cortisol.
The autonomic nervous system changes heart rate and blood pressure during threat or stress. The hypothalamic-pituitary-adrenal axis helps regulate cortisol, a hormone often used as a stress-system marker.
Researchers reviewed whether those systems are tied to experimental pain sensitivity in people with chronic primary pain. The question was specific: do measurable markers such as heart rate, blood pressure, heart-rate variability, and cortisol line up with pain thresholds or pain tolerance in chronic pain groups?
What the Review Counted as Chronic Primary Pain
The review focused on chronic pain conditions that are not fully explained by another diagnosis. Across the 37 studies used in the analysis, researchers separated pain into two broad groups:
- Chronic widespread pain: 653 participants, mostly studies of fibromyalgia.
- Chronic localized pain: 484 participants, including chronic low back pain, chronic neck pain, temporomandibular disorders, irritable bowel syndrome, chronic pelvic pain, and complex regional pain syndrome.
- Typical study design: 33 of the 37 analyzed studies were case-control studies, while 4 were cross-sectional.
- Common pain testing: pressure pain threshold was the most frequent measure, appearing in 21 of the 37 analyzed studies.
The paper also separated stress timing. Some studies measured physiology at rest, some measured it during a stressor, and others measured recovery after stress.
The timing distinction is important because a stable resting heart rate and a delayed recovery after stress can reflect different biological problems.
Blood Pressure Markers Tracked Pain Modulation
The clearest baseline cardiovascular signal involved mean arterial pressure, or MAP. MAP is a combined blood-pressure measure that reflects average pressure across a cardiac cycle.
In the meta-analysis, lower MAP was associated with lower electrical pain threshold and lower electrical pain tolerance. Lower threshold and tolerance mean greater pain sensitivity.
The effect sizes were modest but readable:
- MAP and electrical pain threshold: r = 0.35.
- MAP and electrical pain tolerance: r = 0.30.
- Direction: lower MAP tended to travel with lower tolerance or threshold on those experimental pain tests.
Researchers interpreted this as potentially relevant to baroreceptor-linked pain modulation. In a healthy acute stress response, rising blood pressure can activate pressure sensors that communicate with brainstem pain-control circuits.
In chronic pain, that blood-pressure-related pain dampening can be weaker or less reliable.
Cortisol and Heart Rate Showed Stress-System Links
The HPA-axis finding centered on baseline cortisol. When researchers pooled single morning blood or salivary cortisol measurements, higher cortisol was associated with lower pressure pain threshold.
The meta-analytic correlation was r = -0.22, meaning higher cortisol lined up with greater pressure pain sensitivity.
The autonomic findings were strongest when heart rate was measured around stress. Higher heart rate at baseline was associated with lower pressure pain threshold during a stressor in widespread chronic primary pain.
Higher heart rate during recovery was associated with lower pressure pain thresholds at several time points:
- Baseline pressure pain threshold: r = -0.40.
- Pressure pain threshold during a stressor: r = -0.53.
- Pressure pain threshold during recovery: r = -0.48.
Those recovery results suggest that inefficient post-stress settling may be tied to higher pain sensitivity. The review also found that lower high-frequency heart-rate variability during recovery was associated with lower cold pain tolerance, with r = 0.31.
High-frequency heart-rate variability is commonly used as a marker of parasympathetic activity, which makes the recovery finding consistent with weaker parasympathetic rebound.
Most Possible Links Were Still Not Confirmed
The paper did not report a sweeping stress-explains-pain result. Researchers ran 92 meta-analyses in chronic primary pain populations.
Only 11 produced significant associations. Many possible pairings of stress markers and pain outcomes were not significant.
The mixed pattern argues against using one stress marker as a stand-alone chronic pain biomarker. The findings are better read as a map of plausible systems:
- Cardiovascular regulation: MAP and heart-rate recovery tracked pain sensitivity in some chronic pain groups.
- Parasympathetic recovery: lower HF-HRV after stress marked weaker post-stress settling.
- HPA-axis activity: higher cortisol was linked to lower pressure pain threshold.
- Measurement heterogeneity: different stressors, devices, body sites, and pain tests made direct comparison difficult.
The review also could not settle directionality. Altered stress physiology can increase pain sensitivity.
Persistent pain can disrupt stress physiology, or both systems can reinforce each other over time.
Why Recovery After Stress Carries Mechanistic Weight
The recovery findings are useful for chronic pain mechanisms. A high resting stress marker is one kind of signal. A body that stays physiologically activated after a stressor is another.
In this review, higher heart rate during recovery and lower HF-HRV during recovery were both associated with higher pain sensitivity. That combination fits a model in which chronic pain is partly maintained by sympathetic dominance or reduced parasympathetic reactivation.
It does not prove causation, but it gives future studies a clearer target: measure stress response and pain response repeatedly, not only once at rest.
The next research step is methodological rather than therapeutic. Better chronic pain studies should combine stress markers, standardized pain testing, neural measures, and psychosocial factors across time.
A single blood-pressure or cortisol value is unlikely to explain chronic primary pain by itself.
Citation: DOI: 10.1016/j.neubiorev.2026.106604. Vyverman et al. The stress-pain connection in chronic primary pain: A systematic review and meta-analysis of physiological stress markers in relation to experimental pain responses. Neuroscience & Biobehavioral Reviews. 2026;184:106604.
Study Design: Systematic review and random-effects meta-analysis of physiological stress markers and experimental pain outcomes in chronic primary pain.
Sample Size: 52 studies in the review; 37 studies in qualitative synthesis; 21 studies in meta-analysis; 1,137 chronic pain participants in the analyzed study set.
Key Statistic: Higher recovery heart rate was associated with lower pressure pain threshold at baseline (r = -0.40), during stress (r = -0.53), and during recovery (r = -0.48).
Caveat: Evidence certainty ranged from very low to moderate because studies used small samples, mixed pain groups, and heterogeneous stress and pain measurement methods.