TL;DR: A 2026 open-label feasibility trial in IBRO Neuroscience Reports tested an AI-guided variable levodopa schedule in 5 people with Parkinson’s disease and found 4 patients improved on UPDRS, but the study was far too small and uncontrolled to prove efficacy.
Key Findings
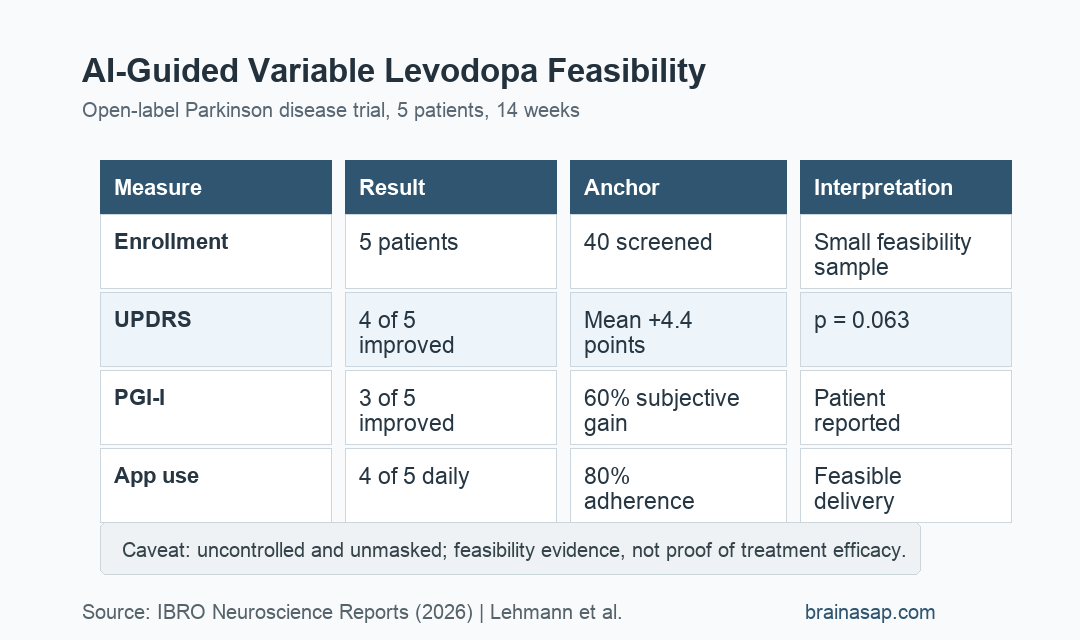
- Feasibility sample: The single-center trial enrolled 5 people with Parkinson’s disease after screening 40 patients.
- 14-week app-guided dosing: Participants used an app that varied levodopa dosing times and doses within predefined physician-approved ranges.
- 80% UPDRS improvement: 4 of 5 patients improved on the Unified Parkinson’s Disease Rating Scale, while 1 patient had no change.
- 4.4-point mean change: Mean UPDRS improvement was 4.4 points, p = 0.063, Cohen’s d = 0.82, 95% CI -0.3 to 9.1.
- 80% daily app use: 4 of 5 participants used the app daily, and all completed follow-up without significant adverse events.
Source: IBRO Neuroscience Reports (2026) | Lehmann et al.
Levodopa remains a core Parkinson’s disease treatment, but long-term use can produce wearing-off periods, on-off fluctuations, and dyskinesias. This small study tested whether controlled variability in dosing could be technically feasible rather than whether the approach should change care now.
The intervention came from the constrained-disorder principle, a framework that treats some biological systems as responsive to structured variability rather than fixed repetition.
AI-Guided Levodopa Dosing Varied Timing and Dose Within Approved Ranges
The trial lasted 14 weeks and was open-label, meaning participants and clinicians knew the intervention was being used. The app generated individualized levodopa schedules by varying timing and dosage inside ranges set in advance.
All 5 participants had Parkinson’s disease and motor fluctuations. The mean age was 66 years, the median disease duration was 5 years, and the mean daily levodopa dose was 656 mg.
- Dosing frequency: Participants averaged 3.6 levodopa dosing times per day at baseline.
- Motor fluctuations: Reported fluctuation duration averaged 2.4 hours per day.
- Baseline severity: Baseline UPDRS total score averaged 42.6.
- Concomitant medications: Some participants also used dopamine agonists, MAO-B inhibitors, COMT inhibitors, or amantadine.
The study did not replace clinician oversight. It tested whether an algorithm-controlled schedule could be implemented and followed by patients in a real treatment context.
4 of 5 Patients Improved on UPDRS
The main clinical measure was the Unified Parkinson’s Disease Rating Scale (UPDRS), a standard rating scale for Parkinson’s motor and non-motor features. 4 of 5 patients improved, and 1 patient had no change.
The mean improvement was 4.4 points. That approached but did not clearly exceed the paper’s cited minimal clinically important difference threshold of 5 points for the UPDRS total score.
- Responder count: 4 patients improved on UPDRS.
- No worsening: No participant had a worse UPDRS score at follow-up.
- MCID threshold: 2 patients exceeded the 5-point minimal clinically important difference threshold.
- Statistical result: The Wilcoxon signed-rank test gave p = 0.063, which did not meet the conventional p < 0.05 threshold.
The effect size was reported as Cohen’s d = 0.82, but effect sizes from a 5-person uncontrolled study are unstable. A single patient’s result can shift the estimate substantially.
Patient-Reported Improvement and App Use Supported Feasibility
The Patient Global Impression of Improvement (PGI-I) scale asked participants to rate subjective change. In this trial, 60% of patients reported subjective improvement.
Adherence was also central because an AI-guided schedule only works if patients can follow it. 4 of 5 participants used the app daily, and all 5 completed the 14-week follow-up period.
- PGI-I improvement: 3 of 5 patients reported subjective improvement.
- Daily app use: 4 of 5 patients used the dosing app each day.
- Completion: All participants completed follow-up.
- Safety: The paper reported no significant adverse events during the study.
These are feasibility outcomes more than efficacy outcomes. They show the approach can be delivered and tolerated in a small group, not that variable dosing outperforms standard levodopa scheduling.
The Open-Label Design Leaves Placebo and Regression Effects Unresolved
The study’s limitations are large and direct. There was no control group, no masking, and only 5 patients. Parkinson’s symptoms also fluctuate naturally, which makes before-after interpretation difficult.
Patients who join a novel app-guided treatment study may be especially motivated, and clinician attention can influence reporting and adherence. Those factors can improve observed outcomes even when the dosing algorithm is not the active cause.
- No randomization: The trial cannot separate algorithm effects from time, attention, expectation, or usual clinical variability.
- No masking: Participants knew they were using a novel personalized dosing system.
- Small sample: With 5 participants, precision is low and subgroup interpretation is not possible.
The fair conclusion is that a randomized, double-masked, adequately powered trial is warranted if the approach is to be tested as a real treatment strategy.
Variable Levodopa Scheduling Remains Hypothesis-Generating
The dosing idea is relevant because fixed drug schedules can lose effectiveness when disease biology, absorption, meals, sleep, and daily activity vary through the day. An adaptive schedule could eventually help some patients, but this trial only establishes early feasibility.
For now, Parkinson’s patients should not change levodopa timing or dose based on this study. Medication timing changes can affect mobility, dyskinesia, sleep, and safety, and they need clinician supervision.
The next evidence step is a controlled trial comparing AI-guided variable dosing with optimized standard dosing, while tracking motor fluctuations, dyskinesia, adherence, quality of life, and adverse events.
Citation: DOI: 10.1016/j.ibneur.2026.02.019. Lehmann et al. A feasibility open-label clinical trial utilizing second-generation artificial intelligence based on the constrained-disorder principle in patients with Parkinson’s disease. IBRO Neuroscience Reports. 2026;20:448-456.
Study Design: Open-label, single-center, proof-of-concept feasibility trial.
Sample Size: 5 people with Parkinson’s disease completed a 14-week AI-guided levodopa dosing intervention.
Key Statistic: Mean UPDRS improvement was 4.4 points, p = 0.063, Cohen’s d = 0.82, 95% CI -0.3 to 9.1.
Caveat: The study had no control group or masking, so it cannot prove that the dosing algorithm caused the observed improvement.