TL;DR: A 2026 preprint in medRxiv reported that a urine beta-amyloid protein test kit separated mild cognitive impairment or Alzheimer’s disease from healthy controls in a multicenter Chinese sample, while a 51,187-person community screen showed age-related positive rates.
Key Findings
- 898-person validation sample: The multicenter case-control arm included 266 healthy controls, 167 people with mild cognitive impairment or Alzheimer’s disease, and 465 non-AD participants with other age-related conditions.
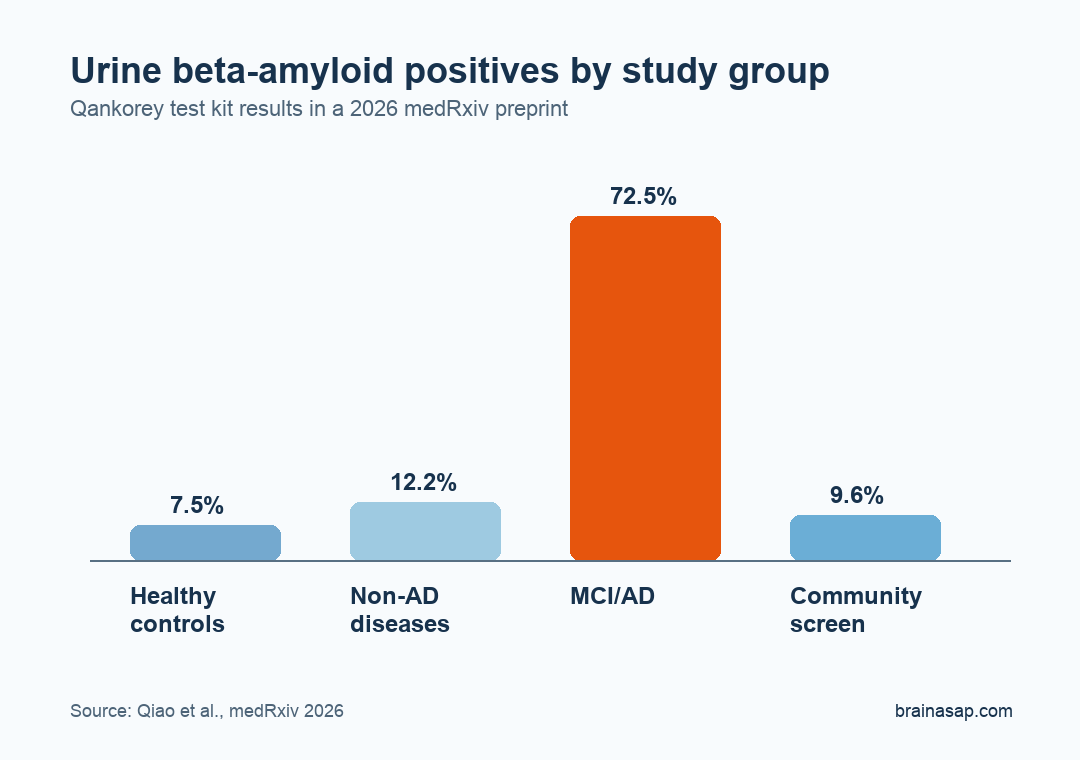
- 72.46% MCI/AD positive rate: Urine beta-amyloid results were weak positive or positive in 121 of 167 MCI/AD participants, compared with 20 of 266 healthy controls.
- 92.5% negative concordance: Against the healthy-control and MCI/AD comparison, the test showed 72.5% positive concordance, 92.5% negative concordance, 84.8% actual concordance, and a kappa value of 0.669.
- 51,187 community tests: In Changsha’s Yuhua District, 4,900 people tested positive, for an overall positive rate of 9.6% among middle-aged and older residents.
- Age gradient reached 15.4%: Community positive rates increased from 6.3% in people younger than 46 to 15.4% in those older than 89.
Source: medRxiv (2026) | Qiao et al.
The study tested a urine beta-amyloid protein detection kit as a lower-burden screening tool for cognitive decline and dementia risk. The kit is not presented as a replacement for clinical diagnosis, amyloid positron emission tomography (PET) imaging, spinal-fluid testing, or blood biomarkers.
Its proposed role is earlier triage in clinics or community settings, where advanced biomarker testing may be too costly or difficult to use as the first step.
Researchers focused on beta-amyloid precursor protein fragments in urine. The paper argues that these urinary fragments may reflect stress or injury in living nerve cells earlier than biomarkers that rise after more advanced neurodegeneration.
Urine Beta-Amyloid Testing Separated MCI/AD From Healthy Controls
The multicenter validation arm enrolled 898 participants across hospitals in China. The main diagnostic comparison was between healthy controls without known age-related disease and participants diagnosed with mild cognitive impairment (MCI) or Alzheimer’s disease (AD).
Results were reported as negative, weak positive, or positive. For the headline clinical comparison:
- Healthy controls: 8 weak positive, 12 positive, and 246 negative results, for a 7.52% weak-positive/positive rate.
- MCI/AD group: 77 weak positive, 44 positive, and 46 negative results, for a 72.46% weak-positive/positive rate.
- Non-AD disease group: 41 weak positive, 16 positive, and 409 negative results, for a 12.23% weak-positive/positive rate.
That spread is the paper’s strongest diagnostic signal. Researchers calculated 72.5% positive concordance, 92.5% negative concordance, 84.8% actual concordance, and kappa = 0.669 when comparing healthy controls with the MCI/AD group.
Kappa measures agreement beyond chance. A value of 0.669 is not perfect, but it falls in the paper’s “good” agreement range and is more useful than a raw positive-rate contrast alone.
Lower Cognitive Screening Scores Had Higher Test-Positive Rates
The study also compared urine test results with two cognitive screens: the Mini-Mental State Examination (MMSE), a brief cognitive test, and the Montreal Cognitive Assessment (MoCA), another brief cognitive test. Neither tool is a stand-alone diagnosis.
Positive rates increased as cognitive scores decreased. That gave the test a severity gradient rather than only a yes/no group difference.
- MMSE gradient: Positive rates increased from 11.8% in the 27-30 range to 74.1% when MMSE was below 10.
- MoCA gradient: Positive rates increased from 8.5% when MoCA was above 25 to 66.7% when MoCA was below 10.
- Repeat-test stability: Among 415 participants with three tests, 391 had consistent first and final results, a 94.2% concordance rate.
This is clinically relevant because a useful screen should not only distinguish diagnosed cases from healthy controls. It should also move in the expected direction as cognitive impairment becomes more severe.
Changsha Community Screening Showed an Age-Related Positive Rate
The larger real-world arm screened 51,187 people in Changsha’s Yuhua District. Overall, 4,900 participants tested positive, producing a 9.6% positive rate.
Age was the clearest community pattern. Positive rates increased across older age groups, which is what researchers would expect from any dementia-risk screen with face validity.
- Younger than 46: 21 of 334 participants tested positive, or 6.3%.
- Ages 60-69: 1,811 of 20,198 participants tested positive, or 9.0%.
- Ages 80-89: 626 of 5,095 participants tested positive, or 12.3%.
- Older than 89: 63 of 409 participants tested positive, or 15.4%.
The follow-up rate was a limitation. Of the 4,900 positive participants, only 449 completed repeat testing.
Only five positive-repeat participants voluntarily underwent subsequent hospital examinations. All five reportedly had brain atrophy or early Alzheimer’s disease, but that number is too small to validate the community-screening program by itself.
Comorbidities and Medications Complicated the Screening Result
The paper’s most practical section examined whether common age-related conditions shifted urine beta-amyloid positivity. In the multicenter sample, memory loss had the strongest association with positive test results, followed by dizziness, hyperlipidemia, stroke history, and hypertension.
The comorbidity analysis is exploratory, but the numbers show why biomarker screening can become difficult in older adults with multiple conditions:
- Memory loss: 102 positive and 112 negative results among those with memory loss, a 47.7% positive rate.
- Hyperlipidemia: 73 positive and 96 negative results, a 43.2% positive rate.
- Stroke history: 22 positive and 32 negative results, a 40.7% positive rate.
- Hypertension: 106 positive and 302 negative results, a 26.0% positive rate.
Medication analyses pointed in the opposite direction for several non-AD treatment categories. Cardiovascular drugs, antithrombotic drugs, and hypoglycemic agents were associated with lower positive rates, but these comparisons were observational and cannot prove that the medications directly reduced dementia biology.
The Preprint Supports Screening Research, Not At-Home Diagnosis
The strongest interpretation is narrow: this urine beta-amyloid kit performed differently in MCI/AD participants, healthy controls, non-AD clinical participants, and a large community screen. The result supports further validation of urine-based screening, especially where PET scans, spinal-fluid testing, or advanced blood assays are not practical first steps.
Several limits should stay visible. The work is a preprint, not yet peer-reviewed, and the community arm had limited clinical follow-up after positive screening.
The clinical groups were not a population-representative sample. The test’s performance against amyloid PET imaging, cerebrospinal fluid biomarkers, or longitudinal dementia conversion was not the main endpoint.
For now, the kit is best read as a candidate triage tool. A positive urine beta-amyloid result would need clinical context, cognitive assessment, and confirmatory testing before it could change care.
Citation: DOI: 10.64898/2026.05.06.26348372. Qiao et al. Real-World Performance of Urine beta-amyloid Test Kits in Multiple Hospital Clinics and Neighborhood Communities of China. medRxiv. 2026.
Study Design: Preprint combining a multicenter case-control validation study and a large community screening program.
Sample Size: 898 clinical participants plus 51,187 community-screened participants in Changsha, China.
Key Statistic: The urine test was weak positive or positive in 72.46% of MCI/AD participants versus 7.52% of healthy controls; kappa was 0.669.
Caveat: The preprint is not peer-reviewed, and the large community screen had limited diagnostic follow-up after positive tests.