TL;DR: A 2026 review in Drug Design, Development and Therapy argued that glucagon-like peptide-1 (GLP-1) receptor agonists, drugs that mimic a metabolic hormone involved in glucose control, have credible brain-protection mechanisms, but clinical evidence for neurological disorders remains mixed.
Key Findings
- 15-page review: Li et al. summarized GLP-1 receptor agonist mechanisms and evidence across neurodegenerative, vascular, inflammatory, psychiatric, seizure, and spinal-cord conditions.
- Four mechanism families: The review emphasized cAMP/PKA/CREB signaling, PI3K/Akt signaling, neuroinflammation control, and AMPK-linked mitochondrial/autophagy effects.
- Parkinson’s trials were mixed: A positive phase 2 exenatide signal was followed by a negative phase 3 result, while lixisenatide showed modest motor benefit in early Parkinson’s disease.
- Alzheimer’s trial evidence was limited: The ELAD liraglutide trial did not significantly change its main brain-glucose-metabolism endpoint, despite exploratory signals.
- Brain entry was a major boundary: The review noted measurable central nervous system penetration for exenatide and lixisenatide, with minimal detectable uptake for liraglutide and semaglutide under normal conditions.
Source: Drug Design, Development and Therapy (2026) | Li et al.
GLP-1 receptor agonists began as diabetes and obesity drugs, but the receptor is also present in brain regions tied to cognition, movement, motivation, and autonomic control.
That receptor distribution has pushed researchers to ask whether the same drug class could help neurological disease.
The review does not present one new trial. It pulls together mechanism work, animal models, and human studies to explain why the drug class looks biologically plausible but not yet clinically settled.
GLP-1 Receptors Give the Drug Class a Brain Rationale
Glucagon-like peptide-1 is a gut hormone involved in insulin secretion, appetite, and gastric emptying. GLP-1 receptor agonists mimic that hormone, with drugs such as exenatide, liraglutide, semaglutide, dulaglutide, lixisenatide, and tirzepatide differing in size, duration, and pharmacokinetics.
Li et al. highlighted a direct anatomical reason for neurological interest: GLP-1 receptors are distributed in the hippocampus, cerebral cortex, hypothalamus, thalamus, amygdala, striatum, nucleus accumbens, and nucleus tractus solitarius.
Those regions are relevant to memory, movement, reward, and autonomic function.
- Metabolic overlap: Type 2 diabetes and obesity share inflammation, oxidative stress, mitochondrial dysfunction, and insulin-signaling problems with several brain disorders.
- Cellular targets: GLP-1 receptor activation can affect neurons, microglia, astrocyte responses, mitochondria, and synaptic plasticity.
- Species differences: Rodent and human receptor distributions are not identical, which limits how directly animal findings translate to patients.
That last point is important for a review article. Strong animal data can justify trials, but it cannot establish clinical benefit by itself.
Four Neuroprotective Mechanisms Repeated Across the Review
The mechanism section centered on four overlapping pathways. First, GLP-1 receptor activation raises cyclic AMP and activates protein kinase A.
That sequence can phosphorylate CREB and increase brain-derived neurotrophic factor (BDNF), a pathway tied to neuronal survival, synaptic strength, and learning.
Second, GLP-1 receptor signaling can activate PI3K/Akt. In Alzheimer-related models, that pathway can reduce GSK-3 beta activity and limit tau hyperphosphorylation, a process involved in neurofibrillary tangles.
Third, the review described anti-inflammatory effects. GLP-1 receptor agonists can reduce overactivated microglia, shift immune signaling away from pro-inflammatory states, and suppress NLRP3 inflammasome activation in some models.
Fourth, the drugs may support mitochondrial function and autophagy through AMPK-related pathways. In neurodegenerative disease, damaged mitochondria and poor protein clearance can worsen neuronal stress.
- Survival signaling: cAMP/PKA/CREB and BDNF pathways support neurons under stress.
- Protein pathology: PI3K/Akt effects may reduce tau-related injury in Alzheimer-relevant models.
- Inflammation control: Microglia and NLRP3 pathways link the drug class to neuroinflammatory disease mechanisms.
- Energy maintenance: AMPK-linked mitochondrial biogenesis and autophagy connect GLP-1 signaling to cellular cleanup.
Parkinson’s and Alzheimer’s Data Were Clinically Mixed
The clearest human trial discussion involved Parkinson’s disease and Alzheimer’s disease. In Parkinson’s disease, the review noted that the positive phase 2 Exenatide PD2 trial was followed by a negative phase 3 Exenatide PD3 trial.
LIXIPARK, a lixisenatide trial, showed modest motor benefits in early Parkinson’s disease.
The trial record is not a clean class win. Drug choice, disease stage, metabolic status, and brain exposure may decide whether a trial can detect benefit.
In Alzheimer’s disease, the ELAD liraglutide trial did not significantly improve the main endpoint of brain glucose metabolism. Exploratory findings may still guide future work, but the review did not treat liraglutide as proven disease-modifying therapy.
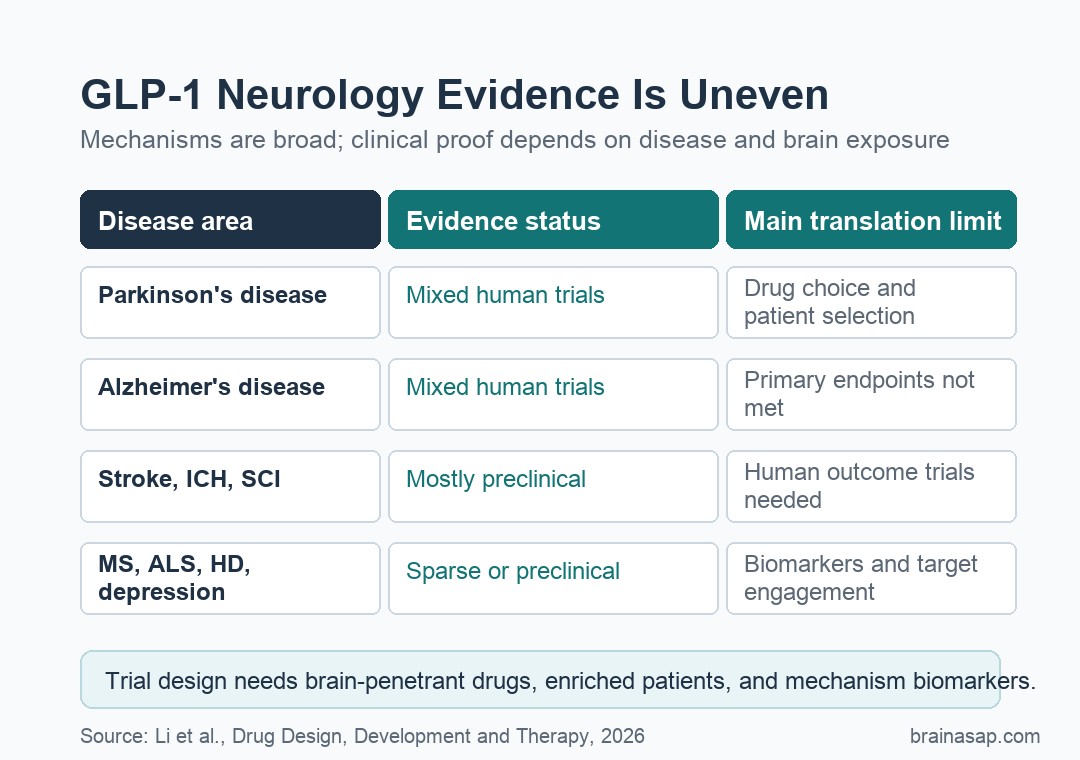
- Parkinson’s disease: Human randomized-trial evidence exists, but findings differ across exenatide and lixisenatide studies.
- Alzheimer’s disease: Trial evidence is active but not yet decisive, especially for primary clinical or metabolic endpoints.
- Other disorders: Stroke, intracerebral hemorrhage, Huntington’s disease, multiple sclerosis, ALS, depression, epilepsy, and spinal-cord injury rely more heavily on animal or sparse clinical data.
Blood-Brain Barrier Penetration May Explain Some Trial Differences
The review’s most useful clinical distinction was drug-specific brain penetration. Exenatide and lixisenatide were described as having measurable central nervous system penetration.
Liraglutide and semaglutide were described as having minimal detectable uptake under normal conditions.
Semaglutide or liraglutide could still affect the brain indirectly through weight, insulin signaling, inflammation, vascular risk, or peripheral metabolism. Trials should not assume that every GLP-1 receptor agonist has the same brain exposure.
This distinction also changes how future trials should be designed. A study of cognition, movement, neuroinflammation, or disease progression needs a drug that reaches the relevant tissue, a population likely to respond, and biomarkers that show whether the intended mechanism was engaged.
- Drug selection: Centrally penetrant agents may be better candidates for direct brain-targeted trials.
- Patient selection: Metabolic status, insulin resistance, disease stage, and inflammatory profile may shape response.
- Outcome selection: Motor scores, cognition, imaging, biomarkers, and functional recovery should match the proposed mechanism.
GLP-1 Neurology Trials Need Biomarkers Before Broad Use
The review supports continued GLP-1 neurology research, not routine neurological prescribing based only on mechanism. Preclinical evidence was broad across AD, PD, stroke, ICH, HD, MS, ALS, depression, epilepsy, and SCI, but the clinical-evidence grade varied sharply by condition.
For patients, the current message is narrower: these drugs have plausible neuroprotective biology and some encouraging human signals, but they are not established disease-modifying treatments for most neurological disorders.
The next useful trials should prioritize brain-penetrant molecules, measure target engagement, and separate metabolic benefit from direct central nervous system action. Without those pieces, a negative trial may reflect the wrong drug, the wrong population, or poor brain exposure rather than a failed biological idea.
Citation: DOI: 10.2147/DDDT.S613616. Li et al. GLP-1 Receptor Agonists in Neurological Disorders: From Mechanisms to Clinical Translation. Drug Design, Development and Therapy. 2026;20:613616.
Study Design: Narrative review of mechanistic, preclinical, and clinical evidence.
Sample Size: Review article; no new patient cohort was enrolled.
Key Statistic: The review contrasted mixed Parkinson’s and Alzheimer’s trial results with broad preclinical benefits across multiple neurological disease models.
Caveat: Clinical conclusions remain condition-specific because many cited benefits are preclinical and GLP-1 receptor agonists differ in brain penetration.