TL;DR: A 2026 medRxiv preprint reported that peripheral blood RNA sequencing separated Parkinson disease from healthy controls and isolated REM sleep behavior disorder more clearly than it separated isolated REM sleep behavior disorder from controls.
Key Findings
- 71 baseline samples: The main analysis included 20 healthy controls, 31 people with isolated REM sleep behavior disorder, and 20 patients with Parkinson disease.
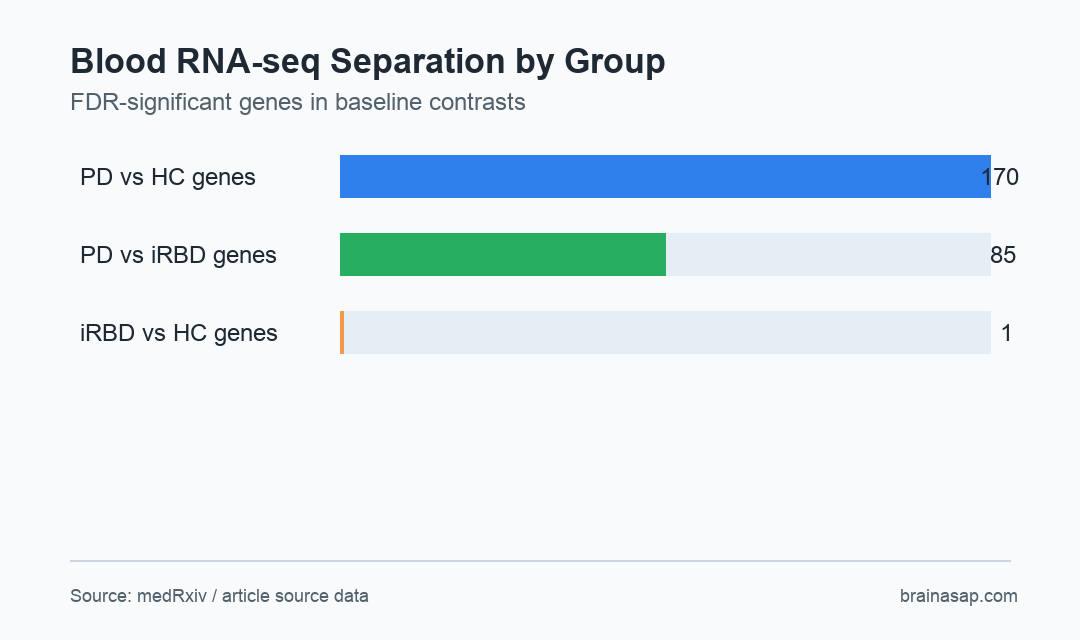
- 170 PD-control genes: Parkinson disease versus healthy control comparison identified 170 FDR-significant genes in peripheral blood RNA-seq.
- 85 PD-iRBD genes: Parkinson disease versus isolated REM sleep behavior disorder identified 85 FDR-significant genes.
- 1 iRBD-control gene: Baseline isolated REM sleep behavior disorder differed weakly from controls, with only one FDR-significant gene.
- 0.883 ROC-AUC: Internal random-forest validation separated Parkinson disease from controls with ROC-AUC 0.883, while control versus iRBD classification was weak.
Source: medRxiv (2026) | Artimovic et al.
Parkinson disease is usually diagnosed after motor symptoms appear, even though biological changes can begin much earlier. Isolated REM sleep behavior disorder, shortened as iRBD, is one of the strongest clinical prodromal markers because many patients later develop Parkinson disease or dementia with Lewy bodies.
The analysis asked a narrower biomarker question: whether ordinary peripheral blood RNA could show a disease-associated transcriptional profile across healthy controls, iRBD, and manifest Parkinson disease. Researchers treated the work as candidate discovery, not as a ready clinical blood test.
Blood RNA-Seq Showed a Stronger Parkinson Disease Signature Than iRBD Signature
The baseline dataset contained 71 independent participants. Follow-up iRBD observations were held aside for exploratory longitudinal analysis rather than mixed into model training.
That separation is important because repeated samples from the same person can make biomarker performance look better than it really is. The preprint explicitly tried to avoid that leakage problem by using baseline samples for model development.
- Healthy controls: 20 baseline samples provided the comparison group.
- Prodromal group: 31 baseline iRBD samples represented people at elevated synucleinopathy risk.
- Manifest disease group: 20 Parkinson disease samples anchored the clinically diagnosed comparison.
- Longitudinal reserve: 19 iRBD follow-up observations, including three post-conversion observations, were used only for exploratory trajectory work.
After adjustment for source dataset, Parkinson disease showed the clearest blood expression signal. The Parkinson disease versus healthy control comparison produced 170 FDR-significant genes, and Parkinson disease versus iRBD produced 85 FDR-significant genes.
The iRBD versus control contrast was much weaker, with only one FDR-significant gene. This finding does not rule out iRBD biology.
It means baseline whole-blood RNA-seq did not identify a uniform prodromal blood profile in this dataset.
The source also helps separate blood biomarker discovery from disease staging. Blood expression may capture immune and systemic biology around Parkinson disease, but it does not directly measure alpha-synuclein pathology in the brain or spinal fluid.
That distinction keeps the interpretation practical. A peripheral RNA panel would need to add information beyond clinical iRBD status, smell testing, autonomic symptoms, imaging, and alpha-synuclein seed amplification assays.
Machine Learning Separated Parkinson Disease Better Than Isolated RBD
The classifier results followed the same pattern as differential expression. Random forest separated healthy controls from Parkinson disease with ROC-AUC 0.883 and balanced accuracy of 0.825.
Parkinson disease versus iRBD classification was similarly strong internally, with logistic regression reaching ROC-AUC 0.889. Control versus iRBD classification was far weaker, with best ROC-AUC of 0.584, close to the kind of performance that should not be read as a clinical classifier.
- PD versus controls: The model correctly classified 17 of 20 controls and 16 of 20 Parkinson disease samples.
- PD versus iRBD: Performance suggested manifest Parkinson disease had a more consistent blood transcriptional state than baseline iRBD.
- Controls versus iRBD: Modest performance fit the weak differential-expression contrast and weakens the case for a simple prodromal diagnostic readout.
The stronger interpretation is therefore not that blood RNA-seq can diagnose prodromal Parkinson disease today. The safer reading is that manifest Parkinson disease carried a reproducible peripheral signature, while iRBD looked biologically mixed.
Internal validation also means the models were tested inside the same study population. A future classifier would need locked features, locked preprocessing, and testing in a separate cohort before any diagnostic performance number becomes clinically meaningful.
PD-Like Projection Scores Suggested Heterogeneous Prodromal Profiles
The longitudinal section explored whether iRBD samples moved toward a Parkinson-like expression profile over time. Projection scores were lowest in healthy controls, highest in Parkinson disease, and mixed among baseline iRBD samples.
Follow-up iRBD samples showed an exploratory upward shift in mean PD-like projection score. Because there were only three post-conversion observations, this part is hypothesis-generating rather than a conversion prediction model.
- Possible early biology: Some iRBD participants may already have peripheral molecular changes closer to Parkinson disease.
- Heterogeneous risk: Other iRBD participants may sit far from the Parkinson-like blood profile at baseline.
- Validation need: External cohorts are needed before any gene panel can be used for prognosis.
The study also prioritized two 24-gene candidate panels, one for Parkinson disease and one exploratory iRBD panel. Those lists are best treated as targets for technical validation and replication, not as final diagnostic products.
Preprint Biomarker Discovery Needs External Validation Before Clinical Use
The main caution is design-related. Whole-blood RNA is shaped by immune-cell mix, medication exposure, inflammation, age, sex, sample processing, and batch effects.
A small discovery cohort can identify promising biology while still overestimating future performance.
The preprint still separates three claims cleanly. Blood transcriptomics detected a manifest Parkinson disease signature, baseline iRBD did not behave as one uniform blood-expression class, and longitudinal iRBD profiling may help identify who is moving toward a Parkinson-like molecular state.
For clinical translation, the next step would be independent testing in larger iRBD cohorts with known phenoconversion outcomes. A blood panel would need to predict future disease beyond known clinical markers, not just distinguish already diagnosed Parkinson disease from controls.
Citation: DOI: 10.64898/2026.06.30.26356917. Artimovic et al. Blood transcriptomics reveals a Parkinson disease signature and heterogeneous prodromal molecular profiles in isolated RBD. medRxiv. 2026.
Study Design: Preprint blood RNA-seq biomarker discovery analysis with differential expression, internal machine-learning validation, and exploratory longitudinal projection.
Sample Size: 71 independent baseline samples plus 19 iRBD follow-up observations.
Key Statistic: Parkinson disease versus control comparison identified 170 FDR-significant genes, while iRBD versus control identified one.
Caveat: This was a small preprint discovery cohort and the proposed panels are not externally validated clinical tests.