TL;DR: A 2026 retrospective analysis posted to medRxiv linked diclofenac and naproxen use in the NACC cohort to lower dementia and Alzheimer disease prevalence, while diclofenac use was also associated with slower Montreal Cognitive Assessment (MoCA) cognitive-screening decline.
Key Findings
- NACC cohort: The analysis used 47,165 National Alzheimer’s Coordinating Center participants with data collected from 2005 to 2022.
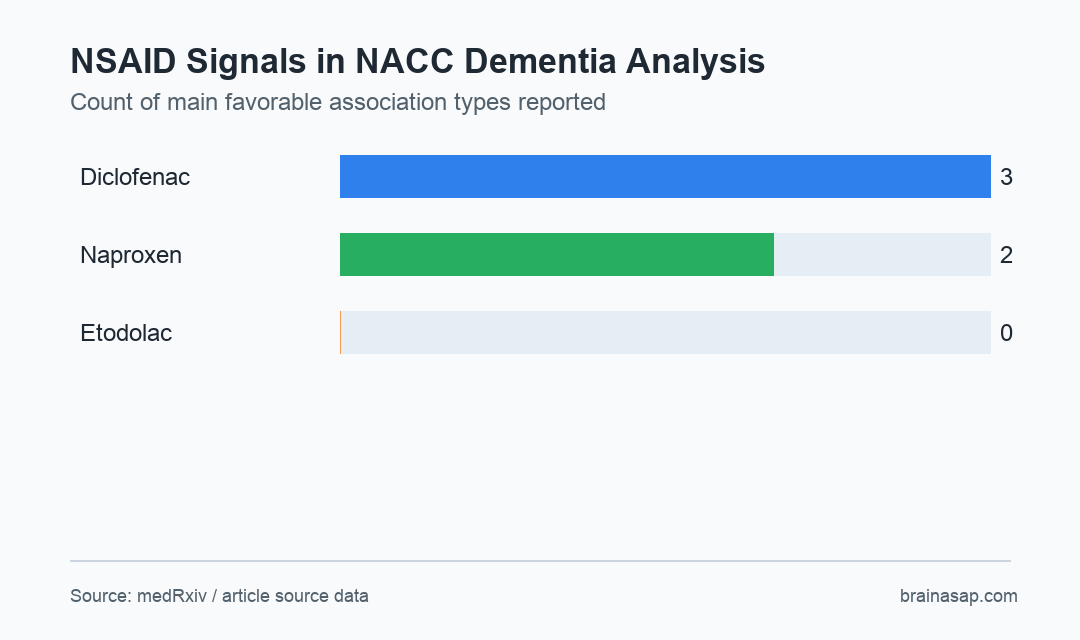
- Diclofenac association: Diclofenac users showed lower odds of dementia and Alzheimer disease than matched non-users.
- Naproxen association: Naproxen use showed similar cross-sectional associations with lower dementia and Alzheimer disease prevalence.
- Etodolac null: Etodolac did not show significant associations with dementia or Alzheimer disease outcomes.
- Slower MoCA decline: Longitudinal modeling associated diclofenac use with a slower decline in Montreal Cognitive Assessment scores.
Source: medRxiv (2026) | Hosseini et al.
Non-steroidal anti-inflammatory drugs, or NSAIDs, have been studied for Alzheimer disease for decades because inflammation is part of neurodegeneration. Past findings have been inconsistent, partly because NSAIDs differ chemically and because observational users are not randomly assigned to a drug.
This analysis revisited the NSAID-dementia link in the National Alzheimer’s Coordinating Center database, using propensity-score matching and longitudinal models. The measured cognitive outcome was the Montreal Cognitive Assessment (MoCA), a brief cognitive screening test.
Diclofenac and Naproxen Had Different Dementia Signals Than Etodolac
The study analyzed 47,165 NACC participants with data collected between 2005 and 2022. Researchers compared selected NSAID users with matched non-users while adjusting for demographic and clinical confounders.
Diclofenac and naproxen showed favorable cross-sectional associations. Both were linked to lower dementia and Alzheimer disease prevalence compared with matched non-users, while etodolac did not show significant associations.
- Diclofenac: Associated with lower odds of dementia and Alzheimer disease and slower cognitive decline in longitudinal models.
- Naproxen: Associated with lower dementia and Alzheimer disease prevalence in cross-sectional comparisons.
- Etodolac: Did not show significant dementia or Alzheimer disease associations in the reported analysis.
- Comparison group: Matched non-users provided the reference group for the main observational contrasts.
The compound-specific pattern is important. A broad claim that all NSAIDs protect the brain would overstate the source.
The supported claim is that diclofenac and naproxen showed associations that etodolac did not.
Drug indication also complicates interpretation. People may take one NSAID rather than another because of pain type, inflammatory disease, clinician preference, insurance coverage, kidney function, cardiovascular risk, or prior side effects.
Those factors can relate to dementia risk on their own. Propensity matching can balance measured variables, but unmeasured prescribing reasons can still influence a retrospective medication analysis.
Diclofenac Was Associated With Slower MoCA Cognitive Decline
The longitudinal part focused on cognitive trajectories using MoCA scores. Diclofenac users had a significantly slower rate of cognitive decline than matched non-users.
That finding gives diclofenac a second type of support in the same dataset: lower disease prevalence at comparison points and slower measured decline over time. It still remains observational, so it cannot prove that diclofenac caused the slower decline.
- Dementia prevalence: Diclofenac and naproxen users were less likely to have dementia than matched non-users.
- Alzheimer disease prevalence: The same two drugs showed lower Alzheimer disease associations.
- Cognitive trajectory: Diclofenac users had slower MoCA decline in longitudinal modeling.
The MoCA detail matters because prevalence can be affected by selection into medication use, clinic attendance, survival, and diagnosis timing. A trajectory analysis adds another angle, although it still depends on how well the model handles confounding.
MoCA also captures a broad cognitive screen rather than one Alzheimer-specific biological process. Slower decline may reflect disease biology, general health differences, medication-selection effects, or combinations of those influences.
Inflammation Biology Is Plausible but Not Proven by the Cohort
The source frames diclofenac as biologically plausible because it may affect inflammatory signaling, including microglial inflammasome pathways. Alzheimer disease involves neuroinflammation, so the mechanism is credible enough to test further.
Credible mechanism is not the same as a treatment recommendation. NSAIDs can cause gastrointestinal bleeding, kidney injury, blood-pressure effects, and cardiovascular risk in some patients. A dementia-prevention article cannot ignore those tradeoffs.
- Mechanistic fit: Anti-inflammatory signaling could intersect with Alzheimer disease biology.
- Clinical risk: Long-term NSAID exposure can harm the gut, kidneys, and cardiovascular system.
- Confounding risk: People who take a particular NSAID may differ from non-users in ways databases cannot fully measure.
- Trial need: Biomarker-defined and risk-stratified studies would be needed before prevention claims are justified.
The clinical reading is therefore cautious. The data help identify diclofenac as a candidate for further Alzheimer disease research, not as an over-the-counter prevention strategy.
A better next step would stratify participants by amyloid, tau, vascular disease, inflammatory markers, and NSAID exposure history. That would test whether any anti-inflammatory association is strongest in a biologically defined subgroup.
Retrospective NACC Data Cannot Establish NSAID Prevention
The strongest limitation is the retrospective design. Propensity matching can reduce measured imbalance, but it cannot randomize medication choice, duration, dose, adherence, indication, or the reasons a clinician avoided NSAIDs in one patient but not another.
Another limitation is outcome context. NACC is a rich Alzheimer disease research dataset, but clinic-based cohorts can differ from the general population.
Medication exposure can also be misclassified if use is intermittent or recorded differently across sites.
The analysis still narrows the next test. Instead of asking whether NSAIDs as a class prevent dementia, future work can ask whether selected compounds, doses, inflammatory profiles, and biomarker-defined Alzheimer disease stages interact with cognitive decline.
Citation: DOI: 10.64898/2026.06.27.26355593. Hosseini et al. NSAID use is associated with lower dementia and Alzheimer disease prevalence and slower cognitive decline: A retrospective longitudinal analysis of the NACC cohort. medRxiv. 2026.
Study Design: Retrospective longitudinal cohort analysis with propensity-score matching.
Sample Size: 47,165 participants from the National Alzheimer’s Coordinating Center database.
Key Statistic: Diclofenac and naproxen were associated with lower dementia and Alzheimer disease prevalence, while diclofenac was also linked to slower MoCA decline.
Caveat: Observational medication data cannot prove that NSAID use prevents dementia or slows Alzheimer disease progression.