TL;DR: A 2026 real-world cohort study in The Journal of Prevention of Alzheimer’s Disease found that lecanemab-treated Alzheimer’s patients had lower Neuropsychiatric Inventory scores over follow-up, and 6-month symptom reductions were associated with regional amyloid-beta positron emission tomography (PET) clearance.
Key Findings
- 144 treated patients: The cohort included people with Alzheimer’s-related mild cognitive impairment or Alzheimer’s dementia who received intravenous lecanemab.
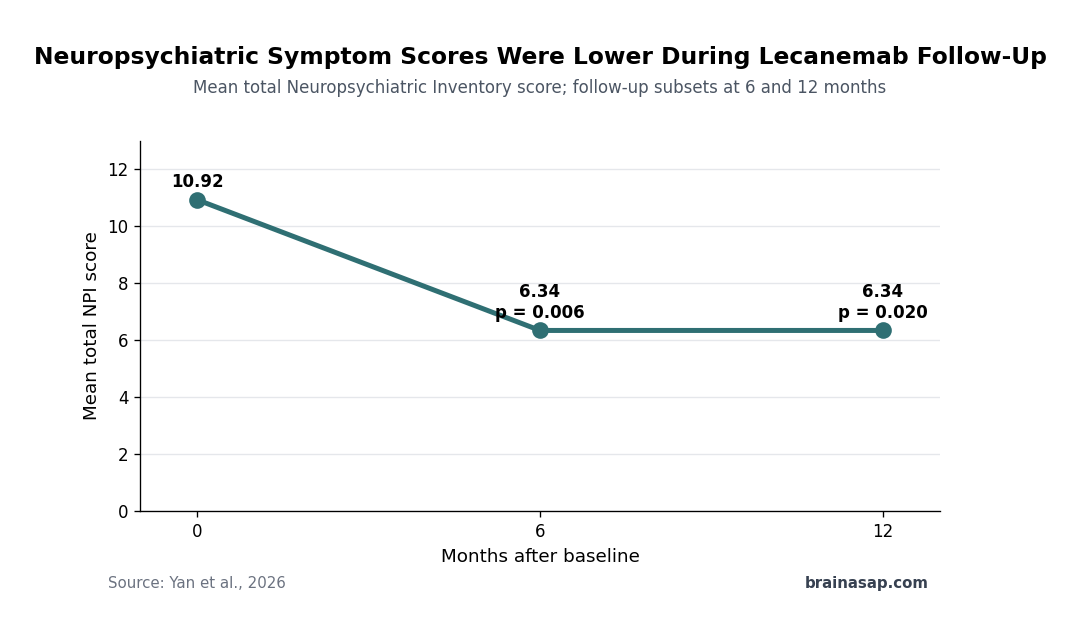
- 6-month NPI drop: Total Neuropsychiatric Inventory scores decreased from 10.92 to 6.34 at 6 months among patients with follow-up data (p = 0.006).
- 12-month NPI drop: In the smaller 12-month follow-up set, total NPI scores decreased from 11.94 to 6.34 (p = 0.020).
- Insular link: Reductions in total NPI score were significantly associated with amyloid-beta clearance in the insular cortex at 6 months.
- Hyperactivity network: Hyperactivity-symptom reductions were associated with amyloid reduction in frontal, temporal, insular, and striatal regions.
Source: The Journal of Prevention of Alzheimer’s Disease (2026) | Yan et al.
Lecanemab is usually discussed around amyloid-beta removal and slowing cognitive decline in early Alzheimer’s disease. This cohort asked a different clinical question: whether neuropsychiatric symptoms such as agitation, hyperactivity, mood symptoms, or psychosis changed during treatment.
The study is not a placebo-controlled trial. It is still useful because neuropsychiatric symptoms are common in Alzheimer’s disease and can drive caregiver burden, disability, medication use, and placement decisions even when cognitive scores are the main trial endpoint.
Lecanemab Cohort Included Mild Cognitive Impairment and Dementia
Researchers enrolled 144 individuals with Alzheimer’s-related mild cognitive impairment or Alzheimer’s dementia. All received intravenous lecanemab and were followed with clinical scales, safety monitoring, and amyloid PET imaging when available.
The baseline cohort included a clinically mixed Alzheimer’s population. By Clinical Dementia Rating, 38.19% had Alzheimer’s-related mild cognitive impairment, 40.97% had mild Alzheimer’s dementia, and 20.83% had moderate Alzheimer’s dementia.
- Clinical visits: Assessments were done at baseline, about 6 months, and about 12 months.
- Behavioral scale: Neuropsychiatric symptoms were measured with the Neuropsychiatric Inventory (NPI), which ranges from 0 to 144, with higher scores reflecting more severe symptoms.
- Imaging readout: Amyloid PET quantified regional amyloid-beta burden across frontal, parietal, temporal, occipital, insular, striatal, and precuneus regions.
Follow-up attrition is important. The 6-month clinical comparison included 73 patients, while the 12-month comparison included 32 patients, so later estimates are based on a smaller subset.
Neuropsychiatric Inventory Scores Fell During Follow-Up
The main behavioral result was a reduction in total NPI score. At 6 months, mean NPI decreased from 10.92 to 6.34, with p = 0.006.
A similar lower score appeared in the 12-month follow-up subset. Mean NPI decreased from 11.94 at baseline to 6.34 at 12 months, with p = 0.020.
- Total symptoms: The total NPI reduction was significant at both measured follow-up points.
- Hyperactivity symptoms: The hyperactivity subsyndrome improved at 6 months, matching the paper’s strongest regional imaging associations.
- Cognitive stability: Mini-Mental State Examination (MMSE), Clinical Dementia Rating (CDR), CDR Sum of Boxes, and activities-of-daily-living measures did not show significant change during the same follow-up windows.
These paired findings do not prove that lecanemab directly treated behavioral symptoms. In this treated cohort, symptom scores moved downward while broad cognitive and functional scales were relatively stable over short follow-up.
Insular Amyloid Clearance Tracked Total NPI Reduction
The imaging analysis asked whether symptom changes related to amyloid-beta clearance in specific regions. At 6 months, total NPI reductions were significantly associated with amyloid-beta clearance in the insular cortex.
The insula is clinically plausible because it participates in salience processing, emotion, interoception, and behavioral regulation. The study’s result is still correlational: it links regional PET change with symptom change, without proving that insular amyloid removal caused the behavioral improvement.
- Total NPI association: The clearest total-score link was with 6-month amyloid-beta clearance in the insular cortex.
- Baseline contrast: Static baseline amyloid measures were not the main behavioral correlate; change in amyloid burden carried the stronger association.
- 12-month caution: The smaller 12-month imaging sample limited the strength of longer-term association testing.
That distinction is important. The finding supports studying dynamic amyloid change alongside behavior, but it does not make one PET region a standalone behavioral biomarker.
Hyperactivity Symptoms Mapped to a Broader Amyloid Network
The hyperactivity subsyndrome showed a wider regional pattern. Symptom reductions were associated with amyloid-beta clearance across the frontal lobe, temporal lobe, insular cortex, and striatum.
Those regions overlap circuits involved in behavioral control, salience, motivation, and emotion regulation. For Alzheimer’s care, the clinical relevance comes from the symptom domain: agitation and hyperactivity can be among the most difficult symptoms for families to manage.
- Frontal regions: Frontal amyloid change may matter for behavioral inhibition and executive control.
- Temporal regions: Temporal-lobe involvement may connect memory, emotion, and social interpretation.
- Striatal regions: Striatal associations fit behavioral activation and motor-restlessness pathways.
- Insular regions: Insular clearance appeared in both total NPI and hyperactivity analyses.
The network language should stay modest. PET associations identify where amyloid change tracked symptom change; they do not show the full causal pathway from antibody treatment to daily behavior.
Safety and Follow-Up Limits Shape the Interpretation
The cohort also tracked adverse events. Infusion-related reactions occurred in 20.83% of participants, and MRI monitoring was used to detect amyloid-related imaging abnormalities during treatment.
2 patients had cerebral infarctions during lecanemab treatment. The researchers described attribution as inconclusive, noting that infarctions were subcortical rather than cortical ARIA-related lesions and that larger studies are needed to clarify risk.
The strongest limitation is design. Without an untreated or placebo comparison group, symptom reduction could reflect regression to the mean, clinical attention, medication changes, caregiver reporting shifts, or selection among patients who remained in follow-up.
The specific takeaway is that behavioral symptoms deserve measurement in anti-amyloid treatment cohorts. This study gives a reason to track NPI domains and regional PET change together, especially when families report agitation, irritability, or other neuropsychiatric changes during treatment.
Citation: DOI: 10.1016/j.tjpad.2026.100600. Yan et al. Reductions in neuropsychiatric symptoms after lecanemab treatment and their associations with imaging markers of beta-amyloid clearance. The Journal of Prevention of Alzheimer’s Disease. 2026;13:100600.
Study Design: Real-world longitudinal cohort of lecanemab-treated Alzheimer’s patients with clinical scales and amyloid PET follow-up.
Sample Size: Baseline cohort included 144 treated patients; 73 had 6-month clinical follow-up and 32 had 12-month clinical follow-up.
Key Statistic: Mean total NPI decreased from 10.92 to 6.34 at 6 months (p = 0.006) and from 11.94 to 6.34 at 12 months (p = 0.020).
Caveat: The cohort lacked a randomized control group, and follow-up samples were smaller than the baseline cohort.