TL;DR: A 2026 Danish register study in British Journal of Health Psychology found that higher divorce conflict was linked to more prescriptions, more primary care visits, and higher hospitalisation odds across the years around legal divorce.
Key Findings
- 1,784 Danish divorcees: Researchers linked divorce-conflict survey data to national registers covering medicine prescriptions, primary care visits, and hospitalisations.
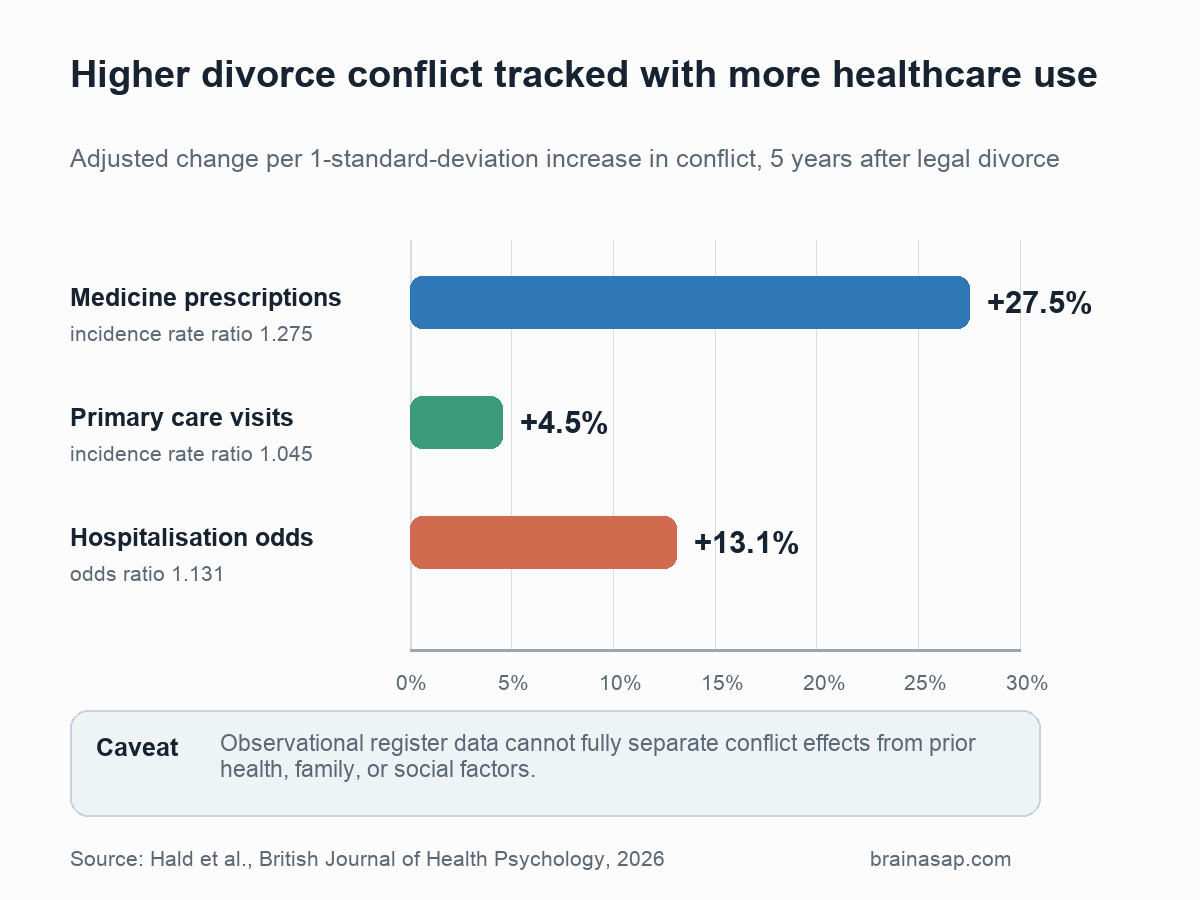
- 28% more prescriptions: A 1-standard-deviation increase in divorce conflict was associated with 27.5% more post-divorce medicine prescriptions.
- 5% more primary care visits: Higher conflict was associated with 4.5% more primary care visits over the 5 years after legal divorce.
- 13% higher hospitalisation odds: Higher conflict was associated with 13.1% higher odds of at least one overnight hospitalisation after divorce.
- 10-year divorce process: High-conflict divorcees already showed worse health trajectories before legal divorce, so the results do not prove conflict alone caused the later healthcare use.
Source: British Journal of Health Psychology (2026) | Hald et al.
Divorce research often treats the legal divorce date like the main event. This study argues for a wider view: health problems can build during the years when the relationship is already breaking down, and conflict may keep pressure on people after the paperwork is finished.
The paper does not say that every difficult divorce causes medical harm. It shows that higher divorce conflict marked a group with consistently heavier healthcare use before and after legal divorce.
Divorce Conflict Was Measured With a Validated Scale
The study used data from 1,784 Danish adults who divorced between 2015 and 2017. Participants completed the Divorce Conflict Scale around the time of juridical divorce, and the researchers linked those scores to Danish national health registers.
The design is important because the health outcomes were not just self-reported symptoms. They came from objective records of filled prescriptions, publicly funded primary care visits, and overnight hospitalisations.
The conflict scale covered three related dimensions:
- Domains of disagreement: Child-rearing, custody, money, emotional issues, and other conflict areas.
- Conflict tactics: Whether disagreements were handled cooperatively or through more hostile strategies.
- Attitudes toward the former spouse: Distrust, negativity, and hostility in the post-separation relationship.
Researchers then treated conflict as a continuous measure. The headline comparisons describe what happened with each 1-standard-deviation increase in conflict, not a simple high-versus-low label.
Higher Conflict Predicted More Prescriptions and Visits
The main analysis counted healthcare use from the divorce date through the next 5 years, while adjusting for earlier healthcare use from 5 to 3 years before divorce. It also adjusted for divorce initiator, age, gender, income, and education.
Higher conflict was associated with increases across all three main health outcomes:
- Medicine prescriptions: Incidence rate ratio 1.275, equal to a 27.5% higher expected count for each 1-standard-deviation increase in conflict.
- Primary care visits: Incidence rate ratio 1.045, equal to a 4.5% higher expected count.
- Hospitalisation: Odds ratio 1.131, equal to 13.1% higher odds of at least one overnight hospitalisation.
The prescription result was the strongest. People at +1 SD conflict had about 8.21 predicted prescriptions across the 5 post-divorce years, compared with 5.05 prescriptions for people at -1 SD conflict.
Primary Care Use Rose Before Legal Divorce
The exploratory trajectory analysis is the most important caution against overreading the study. High-conflict divorcees did not suddenly become medically vulnerable only after the legal divorce date.
For primary care visits, the high-conflict group showed a steeper rise beginning about 2 years before juridical divorce. That supports the idea that divorce is a process, not a single legal moment.
The prescription pattern was also informative. Across conflict groups, prescriptions increased before divorce and then stabilised. High-conflict divorcees had consistently higher prescription levels, while low-conflict divorcees had consistently lower levels.
The paper’s secondary analyses suggested different medication patterns:
- Pre-divorce antidepressants: These accounted for part of the earlier prescription differences between conflict groups.
- Post-divorce psycholeptics: Drugs such as anxiolytics, hypnotics, sedatives, and antipsychotics drove the clearer post-divorce association.
- Psychologist visits: The primary care association was mainly driven by psychologist visits rather than general practitioner or specialist visits.
Those details fit a mixed interpretation. Part of the association may reflect selection, where people already under more strain are more likely to experience high-conflict divorce.
Another part may reflect causation, where conflict adds stress and increases help-seeking.
Hospitalisation Was the Least Clear Outcome
Hospitalisation had a statistically significant main association, but its trajectory pattern was less straightforward. The paper reported relatively stable hospitalisation patterns across the 10-year window and no consistent post-divorce increase in the spline models.
The hospital result is therefore weaker as a conflict-causes-hospitalisation story. People who were hospitalised before divorce may also have been more likely to go through a high-conflict divorce, or unmeasured factors may have shaped both outcomes.
The study adjusted for several important variables, but residual confounding remains plausible. The authors specifically noted missing or difficult-to-separate factors such as personality, social circumstances, children, family estrangement, and parental alienation.
Screening Should Focus on Relationship Strain, Not Blame
The practical takeaway is not that clinicians should medicalise divorce or assign blame to one partner. A more clinically relevant reading is that relationship strain can be part of the context when patients present with stress-linked symptoms, sleep problems, anxiety, or rising healthcare use.
One implication is that primary care could use brief relationship-quality or conflict screeners when patients show stress-related symptoms during a divorce process. Earlier referral to mediation, co-parenting counselling, digital support platforms, or coordinated social care may help more than waiting until the legal divorce is complete.
Several caveats keep the finding bounded:
- Danish setting: Denmark has universal healthcare, liberal divorce laws, and comparatively high social acceptance of divorce, so the results may differ elsewhere.
- Healthcare use is a proxy: More visits and prescriptions can indicate worse health, but they can also reflect appropriate help-seeking.
- COVID-era disruption: Later follow-up years overlapped with the pandemic, which likely reduced some primary care visits.
- Conflict dimensions were combined: The study did not separately test whether conflict topics, tactics, or hostile attitudes had different health links.
Even with those limits, higher conflict tracked with greater healthcare use across the 10-year window. The association makes relationship strain relevant to healthcare screening as well as legal and family support.
Citation: DOI: 10.1111/bjhp.70075. Hald AN, Hald GM, Fallesen P. Divorce conflict and health across the divorce process: A 10-year observational study of medicine prescriptions, primary care visits and hospitalisations. British Journal of Health Psychology. 2026;31:e70075.
Study Design: Longitudinal observational register study of Danish divorcees.
Sample Size: 1,784 adults who divorced in Denmark between 2015 and 2017.
Key Statistic: A 1-standard-deviation increase in divorce conflict was associated with 27.5% more post-divorce medicine prescriptions.
Caveat: The study cannot fully separate conflict effects from pre-existing health, personality, family, or social factors that may shape both conflict and healthcare use.