TL;DR: A 2026 study in eNeuro used intracranial electroencephalography (EEG), a recording method for brain electrical activity, during deep brain stimulation surgery and found that Parkinson’s disease and essential tremor patients with elevated depression symptoms had weaker corticostriatal alpha-beta reward signaling.
Key Findings
- 30 DBS patients participated: The sample included 14 Parkinson’s disease patients and 16 essential tremor patients undergoing deep brain stimulation surgery.
- Depression subgroup was small: Beck Depression Inventory-II scores of 14 or higher classified 5 Parkinson’s patients and 2 essential tremor patients as having elevated depression symptoms.
- Reward increased alpha-beta power: Across patients, reward feedback increased 8-30 Hz alpha-beta power in the caudate and dorsolateral prefrontal cortex.
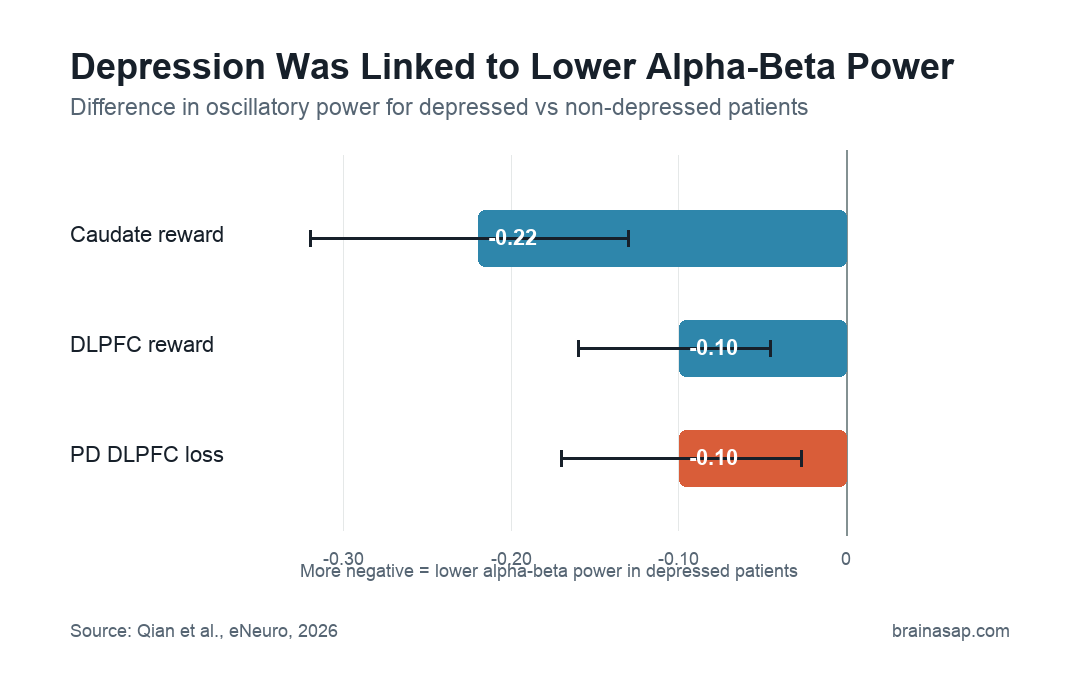
- Depression attenuated reward signaling: Depressed patients had lower reward-related alpha-beta power in the caudate (difference -0.22) and dorsolateral prefrontal cortex (difference -0.10).
- Parkinson’s loss response differed: Depressed Parkinson’s patients had a larger dorsolateral prefrontal alpha-beta decrease after loss feedback than non-depressed Parkinson’s patients.
Depression is common in both Parkinson’s disease and essential tremor, and reward processing is one route by which mood symptoms may connect to movement-disorder circuitry. Anhedonia, or reduced ability to experience pleasure, is especially tied to reward systems.
The measurement setup is the important context. DBS surgery gave researchers temporary access to local field potentials from caudate and prefrontal sites while patients responded to reward and loss feedback.
Source: eNeuro (2026) | Qian et al.
Anhedonia gives the study its clinical frame. If pleasure and feedback learning change in depression, then activity during correct and incorrect task feedback can reveal how mood symptoms reshape learning circuits.
DBS Surgery Created a Rare Window Into Caudate and DLPFC Activity
The study included 30 movement-disorder patients undergoing deep brain stimulation (DBS) surgery. The group included 14 Parkinson’s disease (PD) patients and 16 essential tremor (ET) patients.
Researchers recorded local field potentials from clinical microelectrode hardware while patients completed a working-memory task. Feedback after each response allowed the team to compare brain activity after reward versus loss feedback.
The recording sites were part of corticostriatal circuitry:
- Caudate: A striatal region involved in reward learning, action selection, and cognitive control.
- Dorsolateral prefrontal cortex: The DLPFC, a frontal cortical region involved in working memory and control processes.
- Alpha-beta band: The analysis focused on 8-30 Hz oscillatory power after reward or loss feedback.
Depression symptoms were measured before surgery with the Beck Depression Inventory-II (BDI-II). A score of 14 or higher marked elevated depression symptoms, classifying 5 of 14 PD patients and 2 of 16 ET patients as depressed.
Reward Feedback Increased Alpha-Beta Power in Both Regions
Across the full sample, reward feedback increased alpha-beta power in both recording regions. In the caudate, reward-related alpha-beta power was greater from 340 to 940 ms after feedback appeared.
In the DLPFC, reward-related alpha-beta power was greater from 200 to 900 ms after feedback. The source also reported that DLPFC alpha-beta power decreased after loss feedback, while caudate alpha-beta did not show the same loss-related baseline decrease.
Behavior did not explain the core neural result. Average task performance was 73.8% correct, and working-memory accuracy did not differ between depressed and non-depressed patients.
The feedback pattern can be summarized as follows:
- Reward in caudate: Alpha-beta power increased from baseline, with difference 0.11.
- Reward in DLPFC: Alpha-beta power increased from baseline, with difference 0.054.
- Loss in DLPFC: Alpha-beta power decreased from baseline, with difference -0.047.
- Loss in caudate: The baseline change was not significant.
Depression Was Linked to Weaker Reward-Related Alpha-Beta Power
Depressed patients had lower reward-related alpha-beta power in both the caudate and DLPFC. The caudate difference was -0.22, with a 95% confidence interval from -0.32 to -0.13.
The DLPFC difference was -0.10, with a 95% confidence interval from -0.16 to -0.045. Higher BDI-II scores also predicted lower alpha-beta power after both reward and loss feedback.
For reward feedback, the BDI-II estimate was -0.014 in the caudate and -0.0075 in the DLPFC. Those negative estimates mean higher depression scores tracked with lower alpha-beta power.
Parkinson’s Patients Showed a Stronger Loss-Feedback Difference
The movement-disorder split was limited by sample size, but it added context. Non-depressed PD patients had higher caudate alpha-beta power after reward than after loss, while depressed PD patients did not show that reward-loss separation.
In DLPFC recordings, depressed PD patients had lower alpha-beta power after loss feedback than non-depressed PD patients. The loss-feedback difference was -0.10, with a 95% confidence interval from -0.17 to -0.027.
The ET subgroup was harder to interpret. No depressed ET patients had caudate recordings, and DLPFC loss-related alpha-beta power did not significantly differ between depressed and non-depressed ET patients.
That disease-specific detail keeps the claim narrow. The study supports altered reward and loss signaling in movement-disorder depression, with the clearest loss-feedback finding in PD.
The DBS Sample Makes the Evidence Unusual but Narrow
Intracranial recordings are valuable because they measure local neural activity more directly than scalp EEG. The tradeoff is that the sample is not a broad depression sample; every participant was undergoing DBS surgery for a movement disorder.
The main limitations were concrete:
- No healthy control group: The study could not compare DBS patients with age-matched people without movement disorders.
- Small depressed subgroup: Only 7 patients met the BDI-II depression cutoff.
- Surgical context: Sedation had been stopped before testing, but lingering effects could not be fully excluded.
- Clinical trajectories: Recordings followed DBS electrode paths, so caudate and DLPFC coverage was sparse and not designed like a whole-brain experiment.
- Limited ET caudate data: No depressed ET patients had caudate recordings, restricting diagnosis-by-depression comparisons.
The study provides a mechanistic clue. Depression symptoms in PD and ET patients were linked to altered alpha-beta reward signaling in caudate and DLPFC circuits during a cognitive feedback task.
Future studies would need larger DBS cohorts, broader recording coverage, and treatment follow-up to test whether this alpha-beta pattern can guide therapy.
Citation: DOI: 10.1523/ENEURO.0008-26.2026. Qian et al. Movement Disorder Patients with Depression have Altered Corticostriatal Alpha-Beta Power Response to Reward and Loss. eNeuro. 2026.
Study Design: Intracranial EEG study during DBS surgery, using a working-memory feedback task to compare reward and loss responses.
Sample Size: 30 movement-disorder patients: 14 with Parkinson’s disease and 16 with essential tremor.
Key Statistic: Depressed patients had lower reward-related alpha-beta power in caudate (difference -0.22) and DLPFC (difference -0.10).
Caveat: Only 7 patients met the depression cutoff, all participants were DBS surgery patients, and recording locations were constrained by clinical electrode trajectories.