TL;DR: A 2026 preprint on medRxiv used resting-state functional MRI (fMRI), a brain-connectivity scan taken while people are not doing a task, to divide older adults at Alzheimer’s risk into anxiety biotypes that responded differently to frontal-lobe tDCS stimulation.
Key Findings
- Older-adult tDCS trial: The final sample included 199 older adults, with 99 sham tDCS participants and 100 active tDCS participants.
- Four usable anxiety biotypes: The BETA pipeline identified four interpretable fMRI-connectivity subtypes after excluding one very small 3-person cluster.
- Robust responder pattern: The Robust tDCS Responder subtype showed a statistically significant active-versus-sham advantage for anxiety-score improvement.
- Selective responder caveat: The Selective tDCS Responder subtype had the largest active-stimulation drop in moderate/severe anxiety, but that subgroup included only 3 active participants.
- Connectivity mattered: Responder patterns involved stronger links among lateral occipital, angular gyrus, and frontal control regions.
Source: medRxiv preprint accepted for MIDL 2026 | Stolte et al.
Anxiety in Alzheimer’s disease and related dementias is usually measured with symptom scales and clinical history. Those tools are necessary, but they can group together people whose symptoms arise from different brain-network patterns.
This preprint tested whether resting-state fMRI could separate that mixed group into treatment-relevant subtypes. The specific treatment question was whether older adults at Alzheimer’s risk would show different anxiety responses after transcranial direct-current stimulation (tDCS), a weak electrical stimulation method delivered over the scalp.
The paper is not a clinical rule for choosing tDCS today. It is a proof-of-concept model showing that the same anxiety score may hide different brain-connectivity patterns, and those patterns may matter for who improves after stimulation.
BETA Used Resting-State fMRI to Build Anxiety Biotypes
The researchers introduced BETA, short for Biotypes for tDCS Efficacy in Anxiety. The pipeline started with resting-state fMRI functional connectivity, which measures how strongly brain regions’ activity patterns move together when a person is lying still in the scanner.
The model focused on networks relevant to cognitive aging and anxiety, then compressed those high-dimensional connections into a 50-dimensional embedding. A deep clustering step grouped participants while also using anxiety change after treatment as a clinical guide.
The workflow had three practical pieces:
- Brain-network input: Resting-state fMRI supplied connectivity measures across aging- and anxiety-related networks.
- Clinical outcome guide: State anxiety change helped the model learn clusters tied to treatment response, not only clusters tied to anatomy.
- Subtype output: The resulting biotypes were then tested for sham-versus-active tDCS differences.
That last step is important. A biotype that looks clean on a brain scan has limited value if it does not separate clinically meaningful outcomes.
The Study Included 199 Older Adults at Alzheimer’s Risk
The final dataset included 199 participants after excluding people with missing anxiety or fMRI data. The mean age was 71.27 years, and the sample included 61 males and 138 females.
Participants came from a double-blind tDCS trial. The sample was split almost evenly: 99 people received sham tDCS, and 100 received active tDCS.
Anxiety was measured with the State-Trait Anxiety Inventory state score (STAI-S), a 20-item questionnaire for current anxiety symptoms. Scores were collected at baseline and again after the intervention period.
The tDCS intervention paired frontal-lobe stimulation with cognitive training. Active sessions used stimulation over dorsolateral prefrontal cortex locations, while sham sessions used the same setup without sustained active stimulation.
One Biotype Showed a Clear Active-tDCS Advantage
The model produced five clusters, but one had only 3 participants and was excluded from inferential analysis. The remaining four were labeled Selective tDCS Responder, Robust tDCS Responder, Placebo Responder, and Minimal Responder.
Across the full cluster samples, the strongest active-versus-sham result came from the Robust tDCS Responder subtype. That group showed a statistically significant active-tDCS advantage for state-anxiety improvement, with the paper reporting p = 0.02.
The Robust subtype also showed an active-versus-sham advantage among participants with minimal or mild baseline anxiety, where the reported comparison was p = 0.03. Individual responses still varied, but this fMRI-defined group showed the clearest treatment-linked pattern.
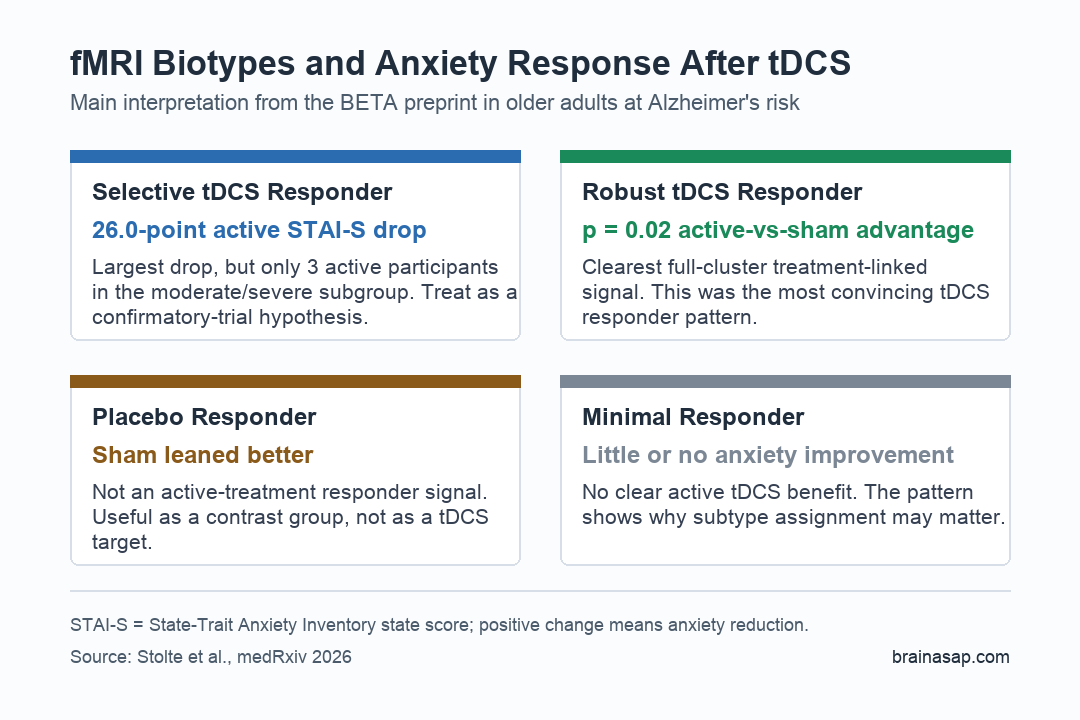
The Largest Anxiety Drop Came From a Tiny Subgroup
The Selective tDCS Responder result needs careful reading. Among participants with moderate or severe baseline anxiety, active tDCS was associated with a mean 26.0-point STAI-S reduction.
That reduction was larger than the paper’s cited 10-point minimal important difference. It is clinically notable, but the active moderate/severe subgroup had only 3 participants.
The table therefore supports a narrow interpretation:
- Large reduction: The selective-responder active subgroup had the biggest anxiety-score drop reported in the main table.
- Small sample: A 3-person subgroup cannot establish a reliable treatment rule on its own.
- Useful hypothesis: The result points to a subtype worth testing in a larger confirmatory trial.
The Placebo Responder subtype also had anxiety-score reductions in moderate/severe participants, but the pattern leaned toward sham and was not the active-treatment response the model was designed to find.
Responder Patterns Involved Visual and Frontal Control Networks
The connectivity analysis pointed to stronger links among sensory-processing and frontal-control regions. The paper highlighted the lateral occipital cortex, the angular gyrus, and frontal regions including superior, inferior, and middle frontal gyri.
Those regions are not random in this context. Visual and attention-related processing can interact with anxiety, and frontal control regions are plausible targets for regulation and neuromodulation.
The proposed responder pattern was most visible in two groups:
- Robust Responders: This subtype showed the clearest statistically significant active-tDCS advantage.
- Selective Responders: This subtype shared some connectivity features and showed the large moderate/severe active-treatment drop.
- Nonresponder contrast: Minimal and placebo-responder patterns did not support the same active-treatment conclusion.
The researchers also tested whether the clinical-guidance term mattered. Their ablation analysis reported that the full model separated anxiety-change clusters better than the version without that term, suggesting the model was not only clustering generic fMRI variation.
fMRI-Guided tDCS Selection Still Needs Larger Trials
The main limitation is sample structure. The dataset came from relatively healthy older adults at risk of Alzheimer’s disease; it was not designed primarily as an anxiety-disorder dataset.
Only a minority of participants had clinically relevant anxiety, and some subtype-by-treatment comparisons were too small for strong inference. The excluded cluster with 3 people is one visible sign of that limitation.
The practical takeaway is cautious: resting-state fMRI may help identify who is more likely to benefit from tDCS for anxiety, but the biotypes need validation in larger anxiety-focused and dementia-risk cohorts before they guide treatment.
Citation: DOI: 10.64898/2026.04.24.26351493. Stolte et al. BETA: Resting-state fMRI Biotypes for tDCS Efficacy in Anxiety Among Older Adults At Risk For Alzheimer’s Disease. medRxiv. 2026.
Study Design: Secondary machine-learning analysis of a double-blind sham-controlled tDCS trial using resting-state fMRI and anxiety-score change.
Sample Size: 199 older adults at risk for Alzheimer’s disease and related dementias; 99 sham tDCS and 100 active tDCS participants.
Key Statistic: Robust tDCS Responders showed a significant active-versus-sham anxiety improvement advantage (p = 0.02); Selective Responders had a 26.0-point active-treatment STAI-S drop in a 3-person moderate/severe subgroup.
Caveat: The source is a preprint, clinically relevant anxiety subgroups were small, and the biotypes need larger confirmatory testing before treatment use.





