TL;DR: A 2026 qualitative analysis in PLOS One used 505 ME/CFS memorial entries to map how systemic neglect, clinical dismissal, social isolation, and personal burden appeared in accounts of illness and death.
Key Findings
- 505 memorial entries: The analysis used the National CFIDS Foundation memorial list, downloaded in October 2024.
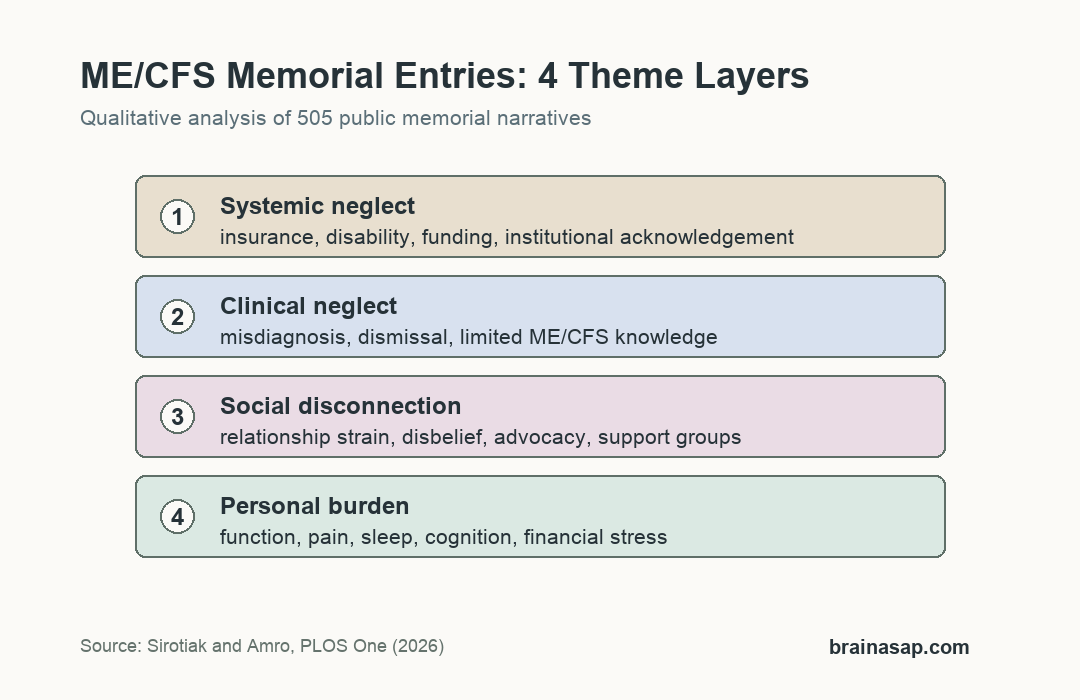
- 4 theme layers: Themes were organized as personal burden, social disconnection, clinical neglect, and systemic institutional failure.
- 2 independent coders: Two coders read and coded each entry before meeting to build themes from the memorial narratives.
- 73.0% female: The memorial sample was mostly female, with an average age at death of 52.5 years.
- 28.3% narrative attribution: Prior quantitative work on the same 505 entries found many deaths were narratively attributed to ME/CFS or its complications.
Source: PLOS One (2026) | Sirotiak and Amro
ME/CFS Memorial Entries Were Treated as Qualitative Illness Narratives
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a disabling chronic illness marked by post-exertional symptom worsening, fatigue, pain, sleep problems, cognitive symptoms, and autonomic symptoms. The condition has often been underdiagnosed, underfunded, and misunderstood.
This study did not recruit living patients or verify medical records. It analyzed public memorial entries submitted by family members, friends, or acquaintances of deceased people who had ME/CFS or related historical labels such as chronic fatigue immune dysfunction syndrome.
That source type shaped the study. Memorial entries can capture grief, advocacy, perceived failures, and lived experience, but they cannot confirm cause of death or diagnostic criteria the way clinical records could.
- Source material: 505 public entries from the National CFIDS Foundation memorial list.
- Data type: secondary qualitative analysis of narrative memorial records.
- Key boundary: acquaintance reports give lived-experience context, not verified epidemiologic cause-of-death data.
505 Entries Produced 4 Interlocking ME/CFS Themes
The memorial list contained 505 entries. Average age at death was 52.5 years, with an age range from 14 to 96. Most listed individuals were female (73.0%) and lived in North America (68.9%).
Two coders independently coded each entry and then discussed interpretations to develop themes. The analysis used an ecological-systems frame, meaning the illness experience was read across individual, relationship, healthcare, and larger institutional levels.
- Personal burden: functional impairment, chronic symptoms, financial stress, and quality-of-life loss.
- Social disconnection: relationship strain, disbelief from others, isolation, support groups, and advocacy.
- Clinical neglect: misdiagnosis, symptom misattribution, dismissal, and ineffective or harmful recommendations.
- Systemic failure: insurance, disability, health-authority, funding, and policy obstacles.
Clinical Dismissal Appeared Alongside Delayed ME/CFS Care
The clinical theme included negative healthcare experiences, lack of clinician knowledge, misattribution of symptoms, and treatment recommendations that entries described as ineffective or harmful. The larger ME/CFS literature also reports long diagnostic delays and inconsistent medical training.
Researchers noted that some estimates suggest up to 90% of people with ME/CFS may be undiagnosed. The memorial entries added narrative detail: disbelief, repeated misdiagnosis, and poor interactions with clinicians could shape whether people sought care at all.
Clinical dismissal was not presented as the only problem. The study connected it to underfunding, limited research investment, scarce specialist care, and disability or insurance barriers.
- Misdiagnosis: entries described symptoms being assigned to other causes before ME/CFS was recognized.
- Misattribution: some narratives described symptoms being treated as psychological rather than medical.
- Care avoidance: negative prior care sometimes contributed to avoidance of later medical contact.
Social Isolation and Advocacy Were Both Common in the Narratives
ME/CFS often limits work, school, family roles, and ordinary social life. In the memorial entries, social strain included disbelief from relatives or acquaintances, divorce or relationship loss, and a sense of being left behind.
The same narratives also described support groups and advocacy. Some people turned to awareness campaigns, online communities, testimony, fundraising, or body donation for research after feeling dismissed by personal, clinical, or governmental systems.
This is one of the study’s strongest qualitative contributions. It shows how illness burden can move across layers: symptoms reduce function, reduced function strains relationships, disbelief increases isolation, and isolation can worsen mental-health risk.
The discussion also linked the memorial narratives to prior ME/CFS research on caregiving burden. In severe ME/CFS, more than 70% of carers have reported providing over 40 hours per week of care, and up to 75% of affected individuals may be unable to work.
Those numbers help explain why financial stress, dependence on others, and housing changes appeared in the entries. The qualitative contribution is the connection between physical symptoms and the social consequences that follow when ordinary independence becomes difficult to maintain.
Mortality Context Requires Careful Interpretation
The study discussed mortality with caution. Earlier work using the same 505-entry list reported cancer, cardiovascular problems, and suicide among frequently reported causes of death, and found that 28.3% of deaths were narratively attributed to ME/CFS or complications of the condition.
Memorial entries also described hopelessness, pain, social isolation, loss of independence, and poor treatment experiences. Those factors are clinically important, especially because suicide risk has been discussed in ME/CFS and chronic pain research.
- Selection bias: people listed on a memorial site may not represent all people with ME/CFS.
- Reporter bias: entries reflect relatives’ or acquaintances’ perceptions and grief.
- Verification limit: medical records and death certificates were not available for this qualitative analysis.
The appropriate reading is not that memorial entries prove a mortality rate. They show how people close to deceased patients described the layers of ME/CFS burden, including systems barriers and mental-health strain.
For clinicians and researchers, the findings support a wider assessment frame. Symptom severity, post-exertional malaise, sleep disruption, pain, cognition, social support, disability access, and suicide risk should not be treated as separate problems when they interact in daily life.
Citation: DOI: 10.1371/journal.pone.0343374. Sirotiak and Amro. Investigating the ME/CFS experience through qualitative analysis of memorial entries. PLOS One. 2026;21(4):e0343374.
Study Design: Secondary qualitative thematic analysis of public ME/CFS memorial entries.
Sample Size: 505 memorial entries from the National CFIDS Foundation memorial list.
Key Statistic: The analysis identified 4 theme layers: systemic neglect, clinical neglect, social disconnection, and personal burden.
Caveat: Memorial narratives are sensitive acquaintance reports and cannot verify diagnosis, cause of death, or population-level risk.





