TL;DR: A 2026 study in BJPsych Open found that closely monitored antidepressant care improved quality of life and reduced societal costs in both PReDicT and usual-care groups, while the PReDicT algorithm added uncertain, country-dependent economic value.
Key Findings
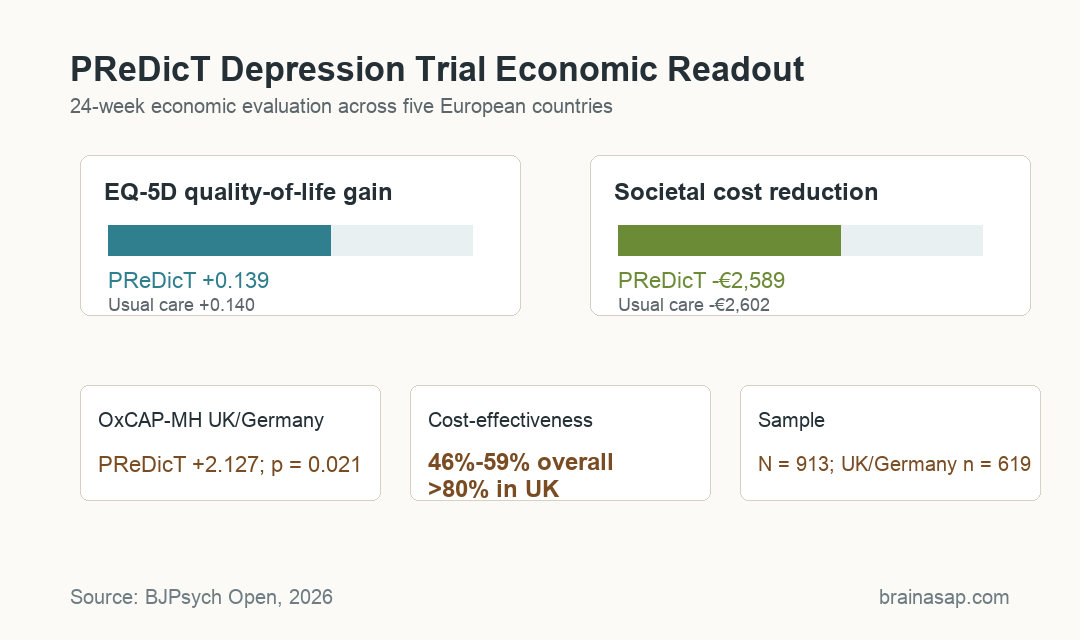
- Multinational trial data anchored the analysis: The economic evaluation followed 913 patients in France, Germany, the Netherlands, Spain, and the UK over 24 weeks.
- Quality-of-life gains were nearly identical: EQ-5D-5L scores increased by +0.139 in the PReDicT group and +0.140 with treatment as usual.
- Societal costs dropped in both groups: Costs fell by €2,589 per participant in PReDicT and €2,602 in treatment as usual.
- Capability improved in two countries: In the UK and Germany subgroup, PReDicT added +2.127 points on OxCAP-MH capability well-being, with p = 0.021.
- Cost-effectiveness was uncertain overall: Trial-level probabilities ranged from 46% to 59%, but exceeded 80% in the UK analysis.
Source: BJPsych Open (2026) | Peric et al.
PReDicT Tested Algorithm-Guided Antidepressant Choice in Primary Care
PReDicT is a digital predictive test designed to guide antidepressant treatment selection by detecting early non-response. The economic paper analyzed whether that algorithm-guided approach offered value compared with treatment as usual.
The evaluation ran alongside the multinational PReDicT randomized controlled trial in five European countries: France, Germany, the Netherlands, Spain, and the UK.
Researchers assessed costs and outcomes over 24 weeks from both health/social care and societal perspectives. Depression economics often needs that broader societal view because lost work, impaired functioning, and caregiver spillover can carry large costs outside medical bills.
The paper measured quality-adjusted life-years using EQ-5D-5L, a standard health-related quality-of-life instrument. In Germany and the UK, it also measured capability-weighted life-years using the Oxford Capabilities Questionnaire-Mental Health (OxCAP-MH), which captures broader functioning and life capability.
Both Depression Care Arms Improved Quality of Life and Costs
The main result was not a simple win for the algorithm. Both groups improved substantially during the trial.
EQ-5D-5L quality-of-life scores increased by +0.139 in the PReDicT group and +0.140 in treatment as usual. Those values were almost identical.
Societal costs also decreased in both groups. The PReDicT arm had a reduction of €2,589 per participant, while treatment as usual had a reduction of €2,602.
The parallel improvement suggests the trial’s closely monitored antidepressant care likely added value regardless of whether the algorithm was used.
The evaluation separated several outcomes:
- EQ-5D-5L: Health-related quality of life improved in both groups by nearly the same amount.
- Societal costs: Both groups showed lower costs during the trial period than before the trial.
- Capability well-being: PReDicT showed an added gain in the UK and Germany subgroup.
The interpretation is therefore narrower than “algorithm beats usual care.” A more accurate reading is that structured antidepressant monitoring improved outcomes, while PReDicT showed capability or productivity value in specific settings.
OxCAP-MH Capability Gains Favored PReDicT in the UK and Germany
The clearest added PReDicT benefit appeared in capability well-being. In the UK and Germany subgroup of 619 participants, PReDicT produced an additional OxCAP-MH gain of +2.127 points, with p = 0.021.
OxCAP-MH is different from a symptom scale. It asks about broader capability and functioning, which can matter when depression treatment helps a person return to work, maintain relationships, or manage daily life more effectively.
The paper links this to the idea that the PReDicT test’s economic value appears to come less from cutting healthcare spending and more from improving functioning and productivity.
That distinction is important for treatment economics:
- Healthcare payer view: A tool can look less attractive if it does not reduce medical costs quickly.
- Societal view: A tool can still matter if it improves work ability, self-management, or everyday functioning.
- Country context: Depression care pathways, resource use, and cost thresholds differed across the five countries.
The UK-specific analysis was the most favorable. Cost-effectiveness probabilities exceeded 80% in the UK, while trial-level probabilities across all settings ranged only from 46% to 59%.
Country-Level Variation Limited the Economic Conclusion
The multinational design was a strength because it tested the intervention across different healthcare systems. It was also a source of uncertainty.
Follow-up completion, outcomes, costs, and depression-care practices varied between countries. The researchers also used UK unit costs for the trial-level analysis because of sample-size and cost-data completeness, which adds another layer of interpretation.
The paper therefore does not support one universal cost-effectiveness claim for PReDicT. It supports a more conditional conclusion: the algorithm looks economically attractive in some systems, especially when capability and productivity gains are counted.
Several limits should shape how readers interpret the result:
- Trial monitoring effect: Both groups likely benefited from close follow-up and measurement-based care.
- Country heterogeneity: Overall estimates combined different healthcare systems and resource-use patterns.
- Economic uncertainty: Trial-level cost-effectiveness probabilities did not show a strong, consistent advantage.
For primary-care depression treatment, that is the most useful finding. Algorithms are not automatically valuable because they are personalized; they have to improve outcomes that matter enough to justify implementation costs.
Close Antidepressant Monitoring May Explain Both-Arm Gains
The strongest practical message is that structured monitoring itself has value. Both PReDicT and treatment-as-usual arms received closely monitored antidepressant care.
Both groups improved beyond expectations for routine care alone.
That fits a broader clinical idea: depression treatment often improves when clinicians track response early, adjust medication when needed, and do not wait months before recognizing non-response.
The PReDicT test remains potentially useful, especially if future studies confirm capability and productivity benefits in specific health systems. But this economic evaluation argues against treating the algorithm as the only active ingredient.
The next question is implementation. A predictive test has to be integrated into appointments, prescribing decisions, patient feedback, and reimbursement rules.
Without that workflow, an algorithm can add complexity without reliably adding value.
Citation: DOI: 10.1192/bjo.2026.11021. Peric et al. The cost-effectiveness of predictive algorithm guided primary antidepressant treatment: economic evaluation of the multinational PReDicT randomised controlled trial. BJPsych Open. 2026.
Study Design: Within-trial economic evaluation alongside a multinational randomized controlled trial.
Sample Size: 913 participants across five European countries; OxCAP-MH capability analysis used 619 UK and Germany participants.
Key Statistic: Trial-level cost-effectiveness probabilities ranged from 46% to 59%, while the UK analysis exceeded 80%.
Caveat: Both trial arms improved, and the algorithm’s added economic value varied by country and analytical perspective.