TL;DR: A 2026 preprint on medRxiv using the Harvard Biomarkers Study found that 43% of Parkinson’s disease patients had depression, anxiety, sleep apnea, or restless legs syndrome, compared with 21% of controls.
Key Findings
- 1,224-person cohort: Researchers analyzed 933 Parkinson’s disease cases and 291 controls in the Harvard Biomarkers Study.
- 43% mood-sleep burden: At least one psychiatric or sleep disorder was present in 43% of Parkinson’s patients versus 21% of controls.
- Restless legs syndrome had OR 4.12: RLS showed the strongest listed association with Parkinson’s disease, with a 95% confidence interval of 1.81 to 12.1.
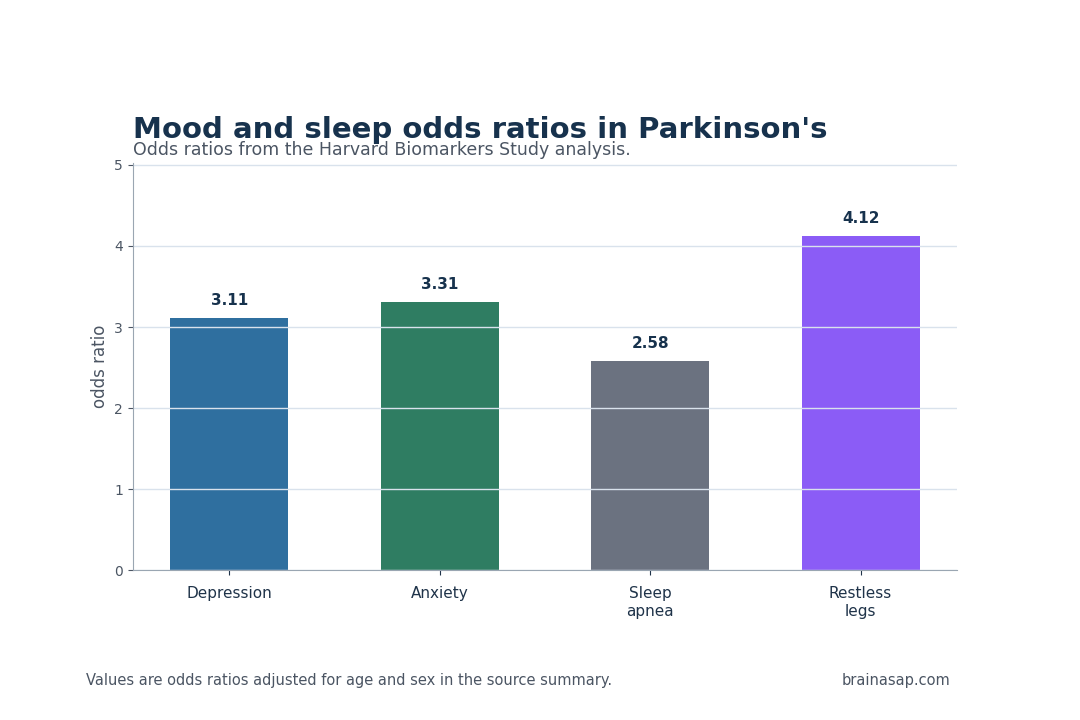
- Depression and anxiety were elevated: Depression had OR 3.11 and anxiety had OR 3.31 after age and sex adjustment.
- Exposure findings also appeared: Pesticide exposure and head trauma were more common in Parkinson’s disease, while smoking was less common.
Source: medRxiv (2026) | Olsen et al.
Parkinson’s Disease Was Linked to a Mood-Sleep Symptom Cluster
Parkinson’s disease is often introduced through tremor, slowness, rigidity, and gait changes.
In clinic, the disease is broader than motor control. Many patients live with mood symptoms, sleep disruption, autonomic symptoms, pain, fatigue, medication effects, and environmental exposures that can shape day-to-day function.
The Harvard Biomarkers Study analysis treated that wider clinical landscape as the main object of study. Researchers examined 64 health features in 933 people with Parkinson’s disease and 291 controls.
After adjusting for age and sex, the most coherent group involved mood and sleep: depression, anxiety, sleep apnea, and restless legs syndrome.
The scale of that cluster was large enough to read clinically. Forty-three percent of Parkinson’s patients had at least one psychiatric or sleep disorder, compared with 21% of controls.
That contrast does not make mood and sleep symptoms diagnostic, but it says they belong in routine Parkinson’s assessment rather than in an optional side conversation.
Depression, Anxiety, Sleep Apnea, and RLS Were More Common
The individual odds ratios give the cluster more shape. Depression was more common in Parkinson’s disease, with an odds ratio of 3.11. Anxiety was similarly elevated, with an odds ratio of 3.31.
Sleep apnea had an odds ratio of 2.58, and restless legs syndrome had the largest reported association among the listed traits, with an odds ratio of 4.12.
Those conditions also correlated with one another. Poor sleep can worsen mood, anxiety can disrupt sleep, and restless legs symptoms can fragment sleep in ways that affect daytime cognition and energy.
The analysis therefore describes more than four separate comorbidities. It describes a linked nonmotor burden that can travel through shared biology, medication effects, activity changes, or disease-related neural systems.
- Depression: OR 3.11, 95% CI 2.1 to 4.71.
- Anxiety: OR 3.31, 95% CI 2.01 to 5.75.
- Sleep apnea: OR 2.58, 95% CI 1.47 to 4.92.
- Restless legs syndrome: OR 4.12, 95% CI 1.81 to 12.1.
For patients, the main point is practical: mood and sleep complaints in Parkinson’s disease should not be brushed aside as unrelated stress.
They can be part of the disease phenotype, and they can affect quality of life even when motor symptoms are being treated.
The odds ratios also help separate routine distress from a disease-linked clinical pattern.
Depression and anxiety can appear after any chronic diagnosis, but the correlated sleep-apnea and restless-legs findings suggest a wider nonmotor package.
In Parkinson’s care, that package can influence fatigue, falls, medication timing, daytime alertness, and caregiver burden.
Those downstream effects can also distort motor assessment. Poor sleep and untreated depression can worsen perceived slowness, reduce exercise tolerance, and lower adherence to therapy.
Treating the nonmotor cluster can therefore improve daily function even when it does not directly slow the neurodegenerative process.
Pesticides, Head Trauma, and Smoking Reproduced Familiar Parkinson’s Links
The same health-phenome screen also captured associations outside mood and sleep.
Pesticide exposure was more common in Parkinson’s disease, with an odds ratio of 1.87. Head trauma was also elevated, with an odds ratio of 2.33.
Smoking was less common among Parkinson’s patients, with an odds ratio of 0.57.
These findings align with long-running Parkinson’s epidemiology, but they serve a useful role inside this study.
They show that the dataset recovered known exposure associations while also identifying a symptom cluster that deserves equal clinical attention.
The supplement-use findings, including higher vitamin D3 and coenzyme Q10 use, are harder to interpret because people with Parkinson’s often change supplement behavior after diagnosis.
- Environmental exposure: Pesticides were associated with higher Parkinson’s odds in this cohort.
- Injury history: Head trauma was more common in Parkinson’s disease cases than controls.
- Behavioral contrast: Smoking showed an inverse association, a recurring observation that should not be interpreted as a health recommendation.
The Parkinson’s Phenome Supports Nonmotor Screening
A phenome-wide approach is valuable because Parkinson’s disease can be clinically crowded.
A neurologist often focuses on gait, tremor, medication timing, and dyskinesia, while mood and sleep problems are split across psychiatry, sleep medicine, and primary care.
The study suggests those features should be considered together.
Screening does not require a complex biomarker.
Asking about depressive symptoms, anxiety, sleep apnea risk, and restless legs symptoms is already feasible in routine visits.
The value is in treating those domains as part of Parkinson’s care rather than waiting for patients to bring them up separately.
A simple clinical screen can also change referrals.
Positive depression or anxiety screening can point toward mental health treatment, while sleep apnea risk can justify sleep-medicine evaluation.
Restless legs symptoms need medication review, iron-status assessment, or targeted therapy depending on the patient’s broader medical picture.
If depression, anxiety, sleep apnea, and RLS cluster together, future studies can test whether they share inflammatory, autonomic, dopaminergic, or circadian mechanisms.
The current analysis cannot settle those pathways, but it gives a reason to stop treating each nonmotor feature as isolated noise.
Cross-Sectional Parkinson’s Data Cannot Settle Cause
The main limitation is design.
The analysis is cross-sectional, so it cannot show whether mood and sleep conditions increase Parkinson’s risk, emerge as early nonmotor signs, follow diagnosis, reflect medication effects, or combine several of those pathways.
Odds ratios describe association, not direction of cause.
The cohort also came from an academic medical center, which does not necessarily represent every Parkinson’s population.
People seen in specialty research settings can differ in disease duration, access to care, medication exposure, supplement use, and willingness to report symptoms.
The supplement findings are a good example of that limitation.
Vitamin D3 and coenzyme Q10 were more common among Parkinson’s patients, but that likely reflects patient behavior after diagnosis, clinician advice, or health-seeking patterns.
It should not be read as evidence that those supplements increase Parkinson’s risk.
Medication exposure also needs careful study.
Dopaminergic treatment can affect sleep, impulse control, and mood, while untreated disease can produce its own psychiatric and sleep symptoms.
Longitudinal data would help separate pre-existing features from symptoms that emerge after diagnosis and treatment.
Even with those limits, the clinical message is grounded: in this large Parkinson’s biomarker cohort, mood and sleep disorders were common, correlated, and quantitatively stronger than a background complaint.
A Parkinson’s visit that ignores depression, anxiety, sleep apnea, and restless legs syndrome is missing a visible part of the disease burden.
Citation: DOI: 10.1101/2022.02.01.22270276; Olsen et al.; Health phenome of Parkinson’s patients reveals prominent mood-sleep cluster; medRxiv; 2026.
Study Design: Cross-sectional health-feature association analysis in the Harvard Biomarkers Study.
Sample Size: 933 Parkinson’s disease cases and 291 controls.
Key Statistic: 43% of Parkinson’s patients had depression, anxiety, sleep apnea, or restless legs syndrome, compared with 21% of controls.
Caveat: Cross-sectional specialty-cohort data cannot determine whether mood and sleep features are causes, early signs, consequences, or mixed pathways.