TL;DR: A 2026 protocol in PLOS One describes a 90-person pilot randomized controlled trial that will test whether virtual reality mindfulness can reduce depression, anxiety, stress, and caregiver burden in family caregivers of people with dementia.
Key Findings
- 90-caregiver pilot: The planned sample includes 90 caregivers of community-dwelling people with dementia in Hong Kong.
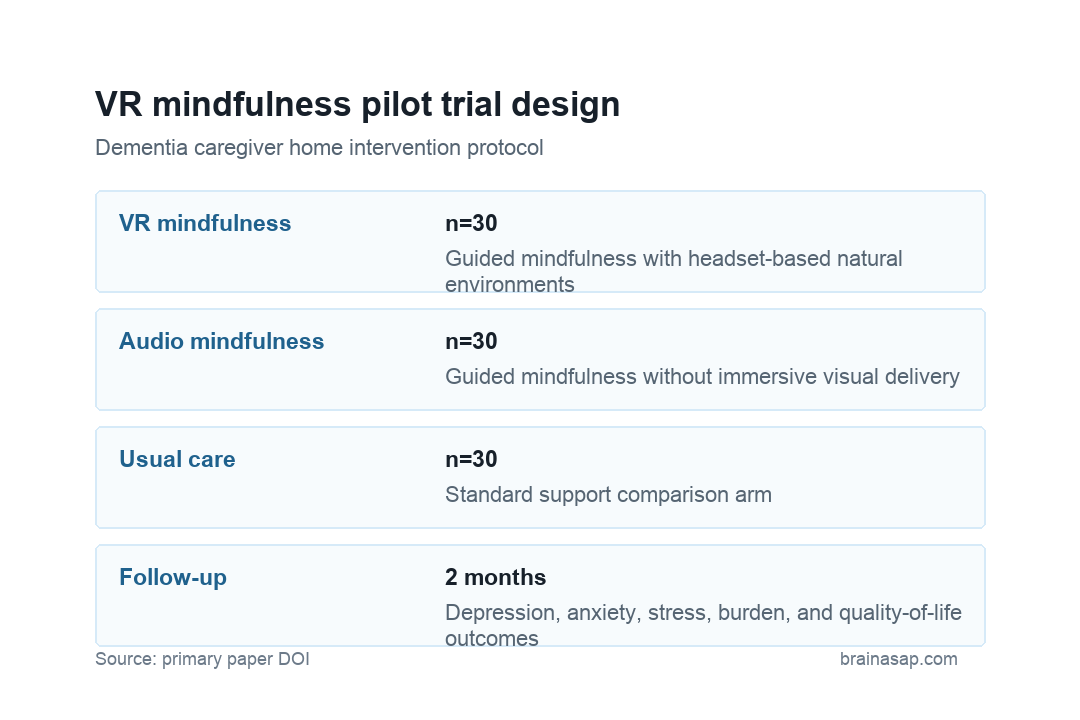
- Three trial arms: Participants will be assigned to virtual reality mindfulness, audio-based mindfulness, or care-as-usual, with 30 caregivers per group.
- Eight-week home program: The virtual reality arm will use a mobile app and headset-based natural environments to support guided mindfulness practice at home.
- Primary mental health outcome: Researchers will measure depression, anxiety, and stress at baseline, after treatment, and at two-month follow-up.
- Protocol caveat: The publication is a trial protocol, so it describes a planned test rather than completed efficacy results.
Source: PLOS One (2026) | Wang et al.
Family dementia caregiving can be relentless. Caregivers often manage safety, medication routines, supervision, finances, appointments, behavior changes, sleep disruption, and emotional distress while still trying to maintain ordinary work and family responsibilities.
Virtual reality mindfulness is being tested as a way to make stress-reduction practice easier to start at home. The intervention uses immersive natural environments and guided exercises, which may reduce distraction and give new meditators a more structured setting than audio alone.
VR Mindfulness Will Be Compared With Audio Mindfulness and Usual Care
The protocol describes a three-arm, parallel, single-blinded pilot randomized controlled trial. Each arm will include 30 dementia caregivers, creating a total planned sample of 90 participants.
Researchers will compare a VR-based mindfulness intervention with an audio-based mindfulness intervention and care-as-usual. That design separates two questions: whether mindfulness practice helps, and whether immersive delivery adds enough engagement or effect beyond an audio guide.
- VR mindfulness: Caregivers practice with a mobile app, headset, guided instructions, and simulated restorative natural scenes.
- Audio mindfulness: Caregivers receive mindfulness instruction without the immersive visual environment.
- Care-as-usual: Caregivers continue standard support and serve as the practical comparison group.
Caregiver Depression, Anxiety, and Stress Are the Primary Outcomes
The primary outcome is psychological status, focused on depression, anxiety, and stress. Secondary outcomes include caregiver burden, mindfulness level, quality of life, and the relationship between caregiver and care recipient.
Assessment timing is straightforward: baseline, post-treatment, and two-month follow-up. Qualitative interviews will also examine feasibility and acceptance, which is important because a digital intervention can fail even when the theory is sound if caregivers do not use it.
Dementia Caregivers Need Home-Based Mental Health Tools
The protocol emphasizes a practical barrier: caregivers often have little free time for clinic-based groups. Mindfulness sessions that require travel, fixed schedules, or long uninterrupted blocks can be difficult for someone responsible for a person with dementia.
Home delivery may reduce that barrier. VR could also standardize instructions and simulate a quieter practice environment, although headset comfort, cybersickness, setup burden, and privacy at home will affect whether the intervention is usable.
The Hong Kong context is also relevant because local caregiver support can be limited, and pandemic-era reports documented high levels of probable depression, anxiety, and stress among dementia caregivers needing flexible help during demanding daily routines at home.
- Adherence measure: The trial can show whether caregivers actually complete an eight-week home program.
- Acceptability check: Interviews can identify whether VR feels supportive, distracting, tiring, or cumbersome.
- Early efficacy signal: Depression, anxiety, stress, burden, and quality-of-life scores can show whether a larger trial is justified.
The Pilot Trial Should Not Be Read as Treatment Proof Yet
Because this is a protocol, the paper does not provide outcome data. It lays out a planned test and explains why the researchers expect VR mindfulness to help caregivers manage distress.
Pilot randomized trials are useful for feasibility, early effect estimates, and trial refinement. They are not usually large enough to settle clinical efficacy, especially when outcomes include subjective distress, caregiver burden, and relationship quality.
That distinction is important for interpreting the headline claim. The protocol’s value is methodological: it defines the groups, timing, outcomes, and qualitative feedback plan needed before anyone can say whether immersive delivery adds clinical benefit.
The planned intention-to-treat analysis also matters. Counting participants in their assigned groups helps preserve the randomized comparison, even when some caregivers miss sessions or stop using the technology.
VR Delivery Could Matter Only If It Reduces Real Caregiver Friction
The most informative part of the eventual study may be whether VR improves practice completion. For caregivers, a technically impressive intervention is not enough.
It must fit into a home where interruptions, fatigue, and care demands are built into the day.
If the VR arm shows better engagement and credible improvement in psychological status, a larger trial could test durability and cost-effectiveness. If it does not, the comparison with audio mindfulness will still clarify whether a simpler tool is enough.
Caregiver interventions also have to be judged by burden. A headset session that requires setup, charging, supervision planning, or recovery from cybersickness could add friction.
A short audio practice may be less immersive but easier to repeat during a difficult week.
The trial is therefore useful even before results are available because it names the operational test. Better caregiver mental health support has to work inside the actual home environment, not only inside a controlled clinic schedule.
Citation: DOI: 10.1371/journal.pone.0347988; Wang et al; A feasibility study on the efficacy of a VR-based mindfulness intervention for dementia caregivers in the home environment: A pilot randomized control trial protocol; PLOS One; 2026;21(4):e0347988.
Study Design: Three-arm, single-blinded pilot randomized controlled trial protocol.
Sample Size: Planned enrollment of 90 dementia caregivers, with 30 per arm.
Key Statistic: No efficacy result yet; the planned primary outcome is depression, anxiety, and stress after an eight-week intervention.
Caveat: Protocols describe intended methods and hypotheses, so completed trial data are needed before clinical claims can be made.