TL;DR: A 2026 review in Current Opinion in Psychiatry found that earlier clozapine use in schizophrenia, especially after early nonresponse or relapse, was linked to better relapse prevention and stronger response rates than repeated nonclozapine antipsychotic trials.
Key Findings
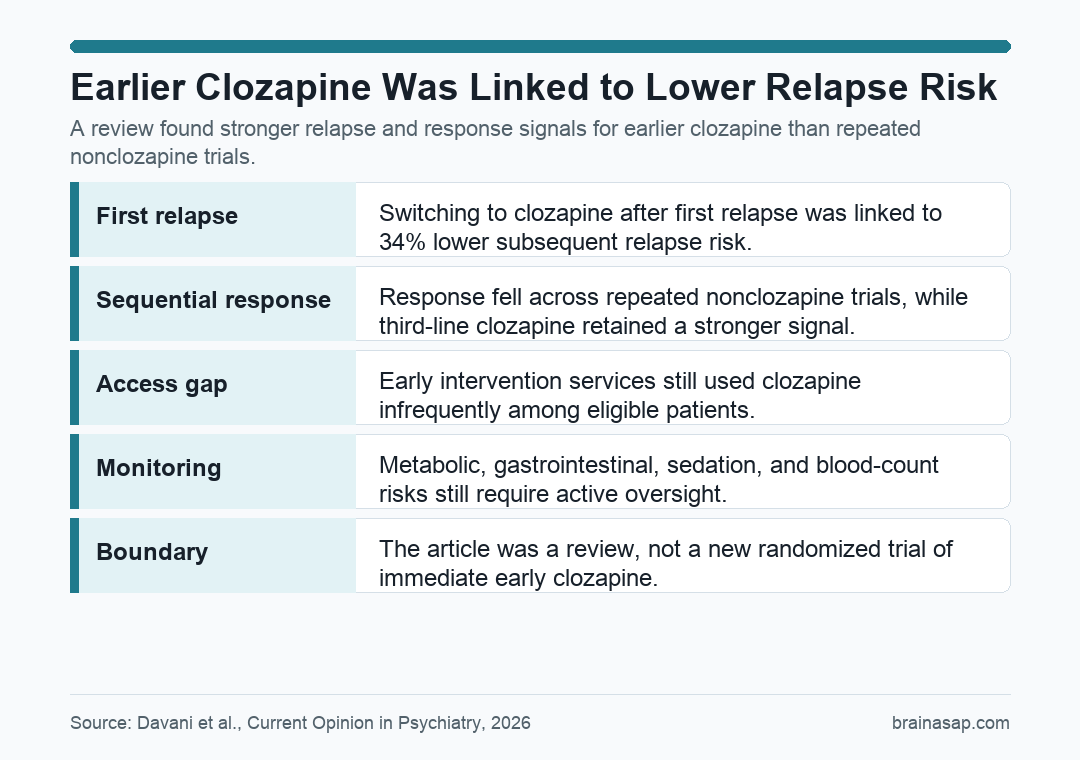
- Relapse prevention improved: Switching to clozapine after first relapse was associated with a 34% lower subsequent relapse risk than continuing nonclozapine treatment.
- Repeated nonclozapine trials weakened: Response fell from 53% on first-line antipsychotic treatment to 26% after a second-line trial.
- Third-line clozapine performed better: In sequential treatment data, third-line clozapine reached 43% response, compared with 26% for another nonclozapine antipsychotic.
- Early access remained rare: In one early intervention service, 30.2% met treatment-resistance criteria, but only 7.8% received clozapine within 2 years.
- Safety concerns still mattered: Sedation, hypersalivation, constipation, metabolic changes, monitoring burden, and nonadherence remained practical barriers.
Source: Davani et al. reviewed recent cohort, registry, randomized, and systematic-review evidence on clozapine in the first 5 years after schizophrenia diagnosis.
Clozapine is usually treated as the medication clinicians reach for after repeated antipsychotic failure. The review argues that this sequence may waste an important early window in schizophrenia care.
Schizophrenia often begins in late adolescence or early adulthood, when school, work, relationships, and independent living are still being built. Relapse during the first few years is common, and repeated episodes can make stable recovery less likely.
The clinical question is not whether clozapine has risks. It does. The question is whether the risks of monitoring, side effects, and clinician hesitation should keep clozapine delayed after early treatment failure.
Early Schizophrenia Relapse Data Favored Clozapine After First Relapse
One of the clearest signals came from a Finnish registry cohort of 3,000 people with first-episode schizophrenia who had a first relapse. Switching to clozapine after that relapse was linked to a 34% lower risk of another relapse than continuing nonclozapine monotherapy.
The 2-year relapse rates made the contrast easier to understand: 57.1% after switching to clozapine versus 73.2% with nonclozapine monotherapy. Clozapine did not prevent relapse for everyone, but it did change the risk curve in a clinically meaningful direction.
For early-stage schizophrenia, relapse prevention is not only a symptom metric. Relapse can mean hospitalization, interrupted education or work, higher family burden, and greater difficulty rebuilding daily routines.
Sequential Antipsychotic Trials Showed Diminishing Returns
The review also summarized sequential treatment data. Response was highest during the first antipsychotic trial and dropped sharply after failure. Across the reviewed evidence, first-stage response was 53%, while second-stage response was 26%.
The sequential pattern is clinically important because many patients are still cycled through several nonclozapine antipsychotics before clozapine is offered. In the sequential-treatment analysis, third-line clozapine reached 43% response, while a third nonclozapine antipsychotic reached 26%.
In first-episode psychosis cohorts, the contrast was even larger: 45% response with third-stage clozapine compared with 15% for another nonclozapine option. The review treats that gap as a reason to reconsider the default delay.
- First trial: Standard antipsychotic treatment still has the highest initial response probability.
- After failure: The expected gain from simply trying another nonclozapine medication falls.
- After repeated failure: Clozapine retains a stronger response signal than another nonclozapine switch.
Clozapine Within 3 Years Was Linked to Negative Symptoms and Functioning
Timing was another central result. In one clozapine-treated cohort, starting clozapine within 3 years of first episode was associated with better negative symptom remission and higher functioning scores.
Negative symptoms include problems such as reduced motivation, blunted emotional expression, and social withdrawal. These symptoms often drive disability and are harder to treat than hallucinations or delusions.
The timing finding did not show the same effect for positive symptom remission. That distinction is useful.
Earlier clozapine may be most relevant for functional recovery and negative-symptom burden, not simply for making every symptom domain respond more strongly.
The review contrasted that early window with routine-care delays. One summarized cohort reported an average of 9.8 years from first episode to clozapine initiation and 47.7 months after treatment-resistance diagnosis.
Underuse Was a System Problem, Not Just a Medication Problem
The gap between eligibility and treatment was large. In a specialized early intervention sample, 30.2% of first-episode patients met treatment-resistance criteria, but only 7.8% received clozapine within 2 years.
Treatment resistance generally means insufficient response after at least two adequate antipsychotic trials. The review’s point is that many patients crossed that threshold without receiving the medication most associated with better outcomes after repeated failure.
Implementation barriers were practical and familiar:
- Monitoring burden: Blood monitoring and side-effect checks make clozapine more labor-intensive than many other antipsychotics.
- Patient hesitation: Some patients refuse the medication, especially when monitoring and adverse effects are not explained clearly.
- Clinician hesitation: Prescribers may delay clozapine because of safety concerns, service logistics, or habit.
- Service design: Dedicated clozapine pathways can shorten initiation delays, while fragmented care can stretch delays across years.
The review noted that specialized early intervention services were able to start clozapine much faster in some settings. That suggests delays are partly modifiable, not inevitable.
Safety Tradeoffs Remained Real but Measurable
Clozapine’s adverse-effect profile still belongs in the center of the decision. The reviewed first-episode and early-stage evidence reported common problems such as sedation, hypersalivation, constipation, and metabolic changes.
One early-phase sample reported metabolic effects in more than 50% of patients, including changes in body mass index and triglycerides. Another randomized contrast found similar short-term response between clozapine and quetiapine, but more somnolence, hypersalivation, and constipation with clozapine.
Short-term serious adverse events appeared uncommon in the reviewed early-stage samples, but discontinuation could still be substantial. One real-world early intervention study reported 35% discontinuation because of adverse events and nonadherence combined.
A balanced reading is straightforward: early clozapine is not a casual escalation. It is a monitored treatment that may be worth considering sooner when repeated nonclozapine trials are unlikely to help enough.
Biomarkers Could Help Select Earlier Clozapine Candidates
The review also pointed to biomarker-guided prescribing as a possible way to reduce guesswork. Three examples were discussed: striatal connectivity from resting-state functional MRI (fMRI), MC4R genotype for weight-gain risk, and HLA-DQB1 genotype for clozapine-related neutropenia or agranulocytosis risk.
Those markers are not yet a complete decision system. Their value would be in combining likely nonresponse to standard antipsychotics with individualized side-effect risk, so earlier clozapine is aimed at patients most likely to benefit and least likely to experience severe harm.
The review connected that idea to the BEEST trial, a multisite study testing biomarker-informed early schizophrenia treatment. If that kind of approach works, clozapine timing could become less dependent on repeated failure and more dependent on measured risk.
- Clinical takeaway: After early nonresponse or relapse, another nonclozapine trial may have a lower expected response than clozapine.
- Safety takeaway: Earlier use still requires active monitoring for metabolic, gastrointestinal, sedation, and blood-count risks.
- System takeaway: Faster access depends on clinic workflows, patient education, prescriber comfort, and monitoring infrastructure.
The review is still limited by the evidence base. The included studies were heterogeneous, many were observational, and follow-up lengths varied.
Those limits make it hard to claim that every early patient with nonresponse should receive clozapine immediately.
The stronger conclusion is narrower: when schizophrenia is still early and standard antipsychotic response has already failed, delaying clozapine for years may cost patients a period when relapse prevention, negative symptoms, and functioning are still more modifiable.
Citation: DOI: 10.1097/YCO.0000000000001059. Davani et al. Clozapine treatment in the early stages of schizophrenia. Current Opinion in Psychiatry. 2026;39:209-215.
Study Design: Scoping review of recent early-stage schizophrenia evidence, including cohort, registry, randomized, systematic-review, and umbrella-review data.
Sample Size: Six included studies, with sample sizes ranging from 63 participants in a randomized trial to 25,983 participants across meta-analytic evidence.
Key Statistic: Switching to clozapine after first relapse was associated with lower subsequent relapse risk than nonclozapine monotherapy (adjusted hazard ratio 0.66; 95% CI 0.49-0.89).
Caveat: Much of the evidence was observational or synthesized from heterogeneous studies, so timing recommendations still need stronger randomized and biomarker-stratified testing.