TL;DR: A 2026 cross-sectional study in Nature and Science of Sleep linked second-trimester sleep disturbance, measured with the Pittsburgh Sleep Quality Index (PSQI), to depressive symptoms, vomiting, diet quality, and several birth-outcome patterns in 2,210 pregnant women in Wuhan, China.
Key Findings
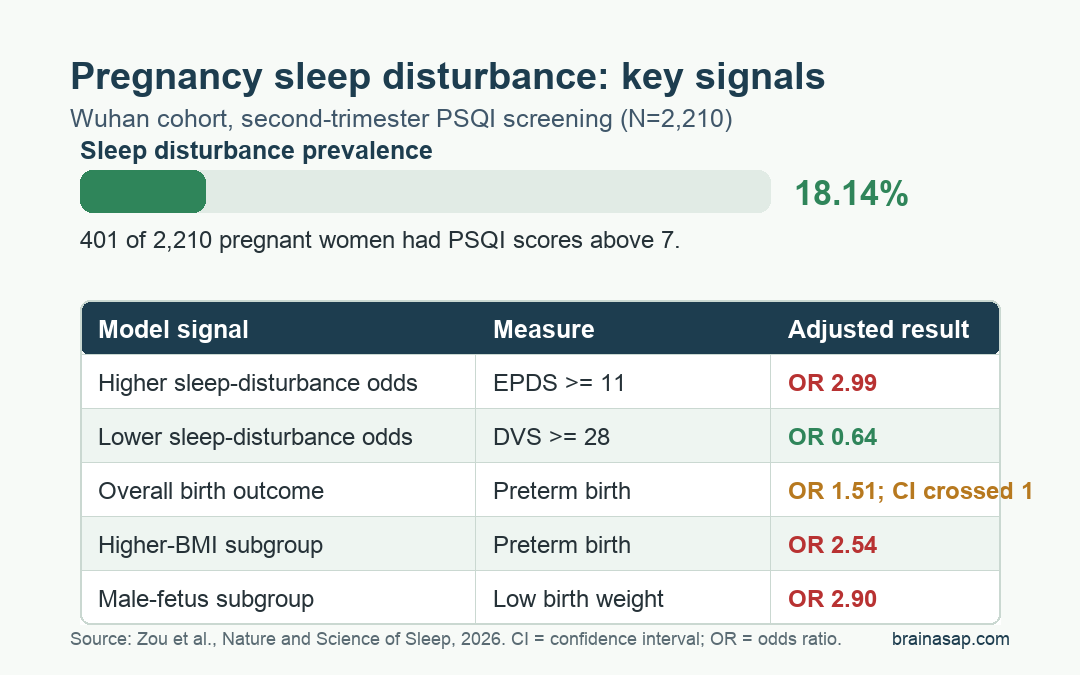
- Sleep disturbance affected 18.14%: 401 of 2,210 pregnant women had PSQI scores above 7 during the second trimester.
- Depression symptoms were the strongest sleep correlate: Edinburgh Postnatal Depression Scale (EPDS) scores of 11 or higher were linked to nearly 3-fold higher odds of sleep disturbance.
- Diet quality moved in the opposite direction: A dietary variety score of 28 or higher was associated with lower odds of sleep disturbance.
- Overall birth-outcome findings were mixed: Sleep disturbance was not significantly tied to preterm birth overall, but it was linked to lower odds of large-for-gestational-age birth and macrosomia.
- Risk patterns differed by subgroup: Sleep disturbance was associated with higher odds of preterm birth and low birth weight among women with pre-pregnancy BMI of at least 24 kg/m2 and among male fetuses.
Source: Zou et al. 2026 Nature and Science of Sleep study.
Sleep problems in pregnancy are common, but the timing matters. Late pregnancy often receives more attention because physical discomfort, fetal movement, and delivery preparation can make sleep harder.
This study focused on the second trimester, when sleep may be easier to screen and when prenatal care still has time to respond.
The researchers studied pregnant women who received routine prenatal examinations at a maternal and child health hospital in Wuhan from July 2023 to March 2024. Women were included if they were adults and were between 14 weeks and 27 weeks plus 6 days of gestation.
PSQI Scores Identified Sleep Disturbance in 401 Pregnant Women
Sleep quality was measured with the Pittsburgh Sleep Quality Index (PSQI), a questionnaire that summarizes sleep quality, latency, duration, efficiency, sleep disturbance, sleeping-medication use, and daytime dysfunction. The study classified women as having sleep disturbance when their PSQI score was above 7.
By that definition, 401 of 2,210 women had sleep disturbance, or 18.14% of the sample. The remaining 1,809 women were in the normal-sleep group.
The study did not find major sleep-group differences for several baseline factors, including age group, education, ethnicity, occupation, income, pre-pregnancy BMI, parity, pregnancy complications, and mid-pregnancy weight gain. The sleep-disturbance group did differ on several health and lifestyle measures:
- Depressive symptoms: High EPDS scores were more common among women with sleep disturbance.
- Diet quality: Higher dietary variety scores were less common in the sleep-disturbance group.
- Pregnancy symptoms: Moderate to severe vomiting was more common among women with sleep disturbance.
- Behavioral factors: Exercise during pregnancy was less common, while pre-pregnancy alcohol consumption was more common.
The EPDS finding is important because the Edinburgh Postnatal Depression Scale is a depression-symptom questionnaire used around pregnancy and postpartum care.
The study cannot determine whether poor sleep worsened mood symptoms, mood symptoms worsened sleep, or both were affected by shared pregnancy stressors. It does show that sleep screening and mood screening were closely connected in this cohort.
Depression Symptoms, Vomiting, and Alcohol History Raised Sleep-Disturbance Odds
After adjustment for demographic, pregnancy, and lifestyle factors, three variables were associated with higher odds of sleep disturbance:
- Depression symptoms: An EPDS score of at least 11 had the largest association, with an odds ratio of 2.99.
- Alcohol history: Pre-pregnancy alcohol consumption had an odds ratio of 1.72.
- Vomiting severity: Moderate to severe vomiting during pregnancy had an odds ratio of 1.81.
Diet quality moved in the other direction. Women with a Dietary Variety Score (DVS) of 28 or higher had lower odds of sleep disturbance than women in the lowest dietary-variety group, with an adjusted odds ratio of 0.64.
These are associations, not proof that changing one factor would automatically repair sleep. Still, they point to a practical prenatal-care cluster.
Sleep complaints, mood symptoms, vomiting burden, diet variety, and exercise are not isolated issues. They can be screened together without treating sleep as a separate lifestyle problem.
Overall Birth Outcomes Showed Mixed Growth Patterns
The researchers then connected second-trimester sleep status with birth outcomes retrieved from the maternal and child health information system. The sleep-disturbance group had slightly lower mean gestational age at delivery, lower birth weight, and lower birth BMI than the normal-sleep group.
For categorical outcomes, the adjusted model did not show a statistically significant overall association between sleep disturbance and several outcomes that might be expected to move upward:
- Preterm birth: The adjusted odds ratio was 1.51, but the confidence interval crossed 1.0.
- Low birth weight: The adjusted odds ratio was 1.48, also not statistically significant overall.
- Small for gestational age: The adjusted odds ratio was 0.81, not a significant increase.
- Small vulnerable neonates: The adjusted odds ratio was 1.10, not a significant overall association.
The statistically significant overall associations went in a different direction. Sleep disturbance was linked to lower odds of large-for-gestational-age birth, with an adjusted odds ratio of 0.65, and lower odds of macrosomia, with an adjusted odds ratio of 0.34.
This result should not be read as evidence that sleep disturbance is protective. It means the overall finding was mixed and may reflect fetal growth, maternal metabolism, subgroup effects, or residual confounding.
BMI and Fetal Sex Changed the Risk Pattern
The clearest risk signal appeared in stratified analyses. Among women with pre-pregnancy BMI of at least 24 kg/m2, sleep disturbance was associated with higher odds of several outcomes:
- Preterm birth: adjusted odds ratio of 2.54.
- Low birth weight: adjusted odds ratio of 2.80.
- Small vulnerable neonate: adjusted odds ratio of 2.41 for the combined category.
Fetal sex also changed the pattern. Among pregnancies with a male fetus, sleep disturbance was associated with higher odds of preterm birth, low birth weight, and small-for-gestational-age birth.
The adjusted odds ratios were 2.15, 2.90, and 1.58, respectively.
Subgroup findings should be read carefully because they divide the sample into smaller groups and can be more sensitive to modeling choices. The study pre-specified BMI and fetal sex as effect modifiers, which helps, but it still cannot prove that sleep disturbance caused these outcomes.
The Study Supports Screening, Not Sleep Blame
Pregnant women should not be blamed for poor sleep. Pregnancy sleep is shaped by symptoms, stress, physiology, work, family demands, and care access.
In this study, the sleep-disturbance group also had more depressive symptoms and more moderate to severe vomiting, both of which are clinical signals rather than simple habits.
For prenatal care, the findings support a low-burden screening approach. A clinic that asks about sleep quality can also ask about mood symptoms, vomiting severity, diet variety, and exercise in the same visit.
That may be especially useful for women with higher pre-pregnancy BMI, where the subgroup analysis showed stronger links with preterm birth and low birth weight.
The caveat is design. This was a single-center cross-sectional analysis of sleep quality during mid-pregnancy, with later birth outcomes drawn from records.
It can identify associations, but it cannot separate cause, reverse causation, and unmeasured confounding.
The strongest conclusion is that second-trimester sleep disturbance may flag a broader maternal-health risk profile that deserves attention before delivery.
Citation: DOI: 10.2147/NSS.S573867. Zou et al. Factors Affecting Sleep Quality in Pregnant Women During the Second Trimester and Its Association with Birth Outcomes. Nature and Science of Sleep. 2026;18.
Study Design: Single-center cross-sectional sleep-quality analysis with birth outcomes retrieved from clinical records.
Sample Size: 2,210 pregnant women in Wuhan, China, assessed during the second trimester.
Key Statistic: Sleep disturbance affected 18.14% of participants and was linked to EPDS scores of 11 or higher with an adjusted odds ratio of 2.99.
Caveat: The design identifies associations and subgroup patterns, not whether sleep disturbance directly caused birth outcomes.





