TL;DR: A 2026 study in Psychological Medicine found that cognitive reserve in non-affective first-episode psychosis was higher with greater genetic predisposition to educational attainment and lower with earlier psychosis onset or family history of psychosis.
Key Findings
- 174 first-episode patients: Researchers analyzed people with non-affective first-episode psychosis, with a mean age of 25.5 years.
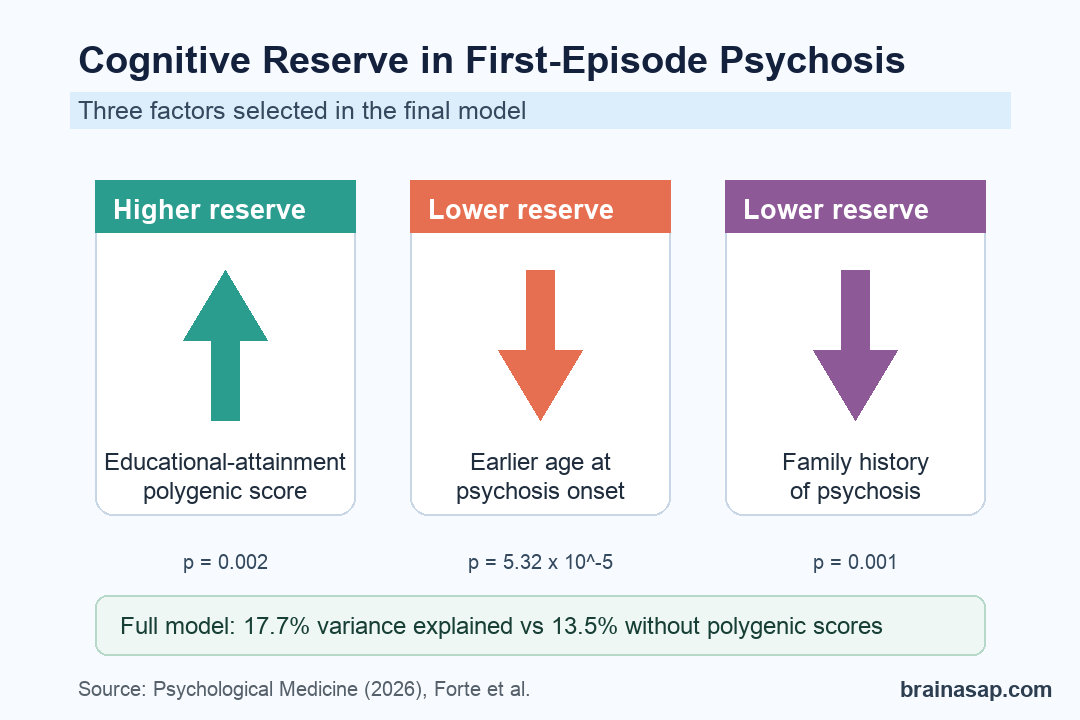
- Educational-attainment genetics stood out: A higher polygenic score for educational attainment was associated with higher cognitive reserve (p = 0.002).
- Earlier onset tracked lower reserve: Younger age at psychosis onset was one of the strongest clinical contributors to lower cognitive reserve (p = 5.32 x 10^-5).
- Family history mattered: A positive family history of psychosis was associated with lower cognitive reserve (p = 0.001).
- Full model explained 17.7%: Adding genetic, clinical, and environmental variables explained 17.7% of cognitive-reserve variance, compared with 13.5% without polygenic scores.
Source: Psychological Medicine (2026) | Forte et al.
Cognitive reserve is the brain’s ability to keep functioning despite illness, stress, or structural vulnerability. In first-episode psychosis, reserve can matter because early symptoms often arrive during school, work, and social-development years.
Researchers examined whether reserve in non-affective first-episode psychosis was mostly tied to clinical timing, family background, environmental markers, or genetic liability measured through polygenic risk scores.
Cognitive Reserve Was Measured as a Socio-Behavioral Proxy
The study included 174 people with non-affective first-episode psychosis from the Spanish PEPs cohort. Non-affective first-episode psychosis means a first psychotic episode not primarily classified as bipolar disorder or major depression with psychotic features.
Researchers did not measure reserve with a single brain scan or memory test. They used a socio-behavioral proxy built from reserve-related life factors that usually reflect educational, occupational, and cognitive enrichment.
- Genetic measures: Polygenic scores were calculated for educational attainment, intelligence, cognitive performance, occupational attainment, physical activity, and schizophrenia.
- Clinical timing: Age at onset was included because earlier psychosis can interrupt education, work, and other reserve-building experiences.
- Family background: Researchers included family history of psychosis as a clinical marker that can also reflect inherited vulnerability.
- Environmental markers: Socioeconomic status and birth weight were tested as non-genetic contributors.
A polygenic score is not a diagnostic test. It is a summary of many common genetic variants, each usually carrying a tiny association with a trait in prior genome-wide studies.
Educational-Attainment Genetics Was the Clearest Polygenic Contributor
Among the genetic scores, the educational-attainment polygenic score had the clearest relationship with cognitive reserve. Higher PRS for educational attainment was linked with higher reserve in both univariate and multivariable analyses.
The univariate estimate for educational attainment was 2.512 with a 95% confidence interval from 0.862 to 4.163 (p = 0.003). In the final multivariable model, the association remained significant at p = 0.002.
Other genetic scores were weaker. The polygenic score for cognitive performance was significant in the univariate analysis, but educational attainment was the polygenic score that remained in the selected full model.
- Educational attainment: The strongest polygenic contributor to reserve in the final model.
- Cognitive performance: Significant in the univariate analysis, but not the final selected multivariable model.
- Schizophrenia liability: Not significantly associated with cognitive reserve in the univariate test.
- Occupational attainment and physical activity: Neither score showed a significant reserve association in the main univariate analysis.
Earlier Psychosis Onset and Family History Pointed the Other Way
Clinical factors also mattered. Earlier age at onset was associated with lower cognitive reserve, while later onset tracked higher reserve. In the final model, age at onset was significant at p = 5.32 x 10^-5.
Family history of psychosis also pointed toward lower reserve. The final model found a significant association at p = 0.001, and the univariate estimate was -6.487 with a 95% confidence interval from -10.977 to -1.996.
These two findings are clinically important because they are not simple lifestyle variables. Earlier onset can reduce reserve by interrupting school, work, and social activity, but it may also reflect stronger neurodevelopmental vulnerability.
- Earlier onset: Psychosis that begins sooner can disrupt reserve-building opportunities while cognitive development is still unfolding.
- Family history: Familial psychosis risk may capture inherited cognitive vulnerability, shared environment, or both.
- Clinical interpretation: Lower reserve should not be treated as a personal failure; it may reflect a mix of timing, family risk, and developmental exposure.
Genetic Data Added a Modest Amount of Predictive Power
The full model combining genetic, clinical, and environmental variables explained 17.7% of cognitive-reserve variance. A model without polygenic scores explained 13.5%.
Adding the educational-attainment polygenic score improved adjusted R2 by 0.042 and improved root mean squared error by 0.288. That is a measurable gain, but not enough to make genetics a standalone clinical tool.
- What the model adds: Genetic liability to educational attainment contributed information beyond age at onset and family history.
- What it does not prove: The study does not show that a genetic score can classify individual patients with enough accuracy for treatment decisions.
- Why family history is complicated: Family history sits between clinical information and inherited liability, so separating genetic from non-genetic explanations is not clean.
Reserve Screening Could Help Target Support Earlier
Early support matters more than genetic determinism. Patients with first-episode psychosis, earlier onset, family history, and low reserve may need more active cognitive, educational, and functional rehabilitation planning.
Because the study is observational, the result should be read as a risk-characterization finding. It supports careful assessment of reserve-related factors, but it does not prove that changing one factor will necessarily raise reserve.
For clinical teams, the lower-reserve profile is concrete: age at onset, family history, and educational-attainment genetic liability identified patients who may need more intensive cognitive and functional support. Those markers may also help researchers design sharper early-intervention studies.
Citation: DOI: 10.1017/S0033291725101360. Forte MF et al. Cognitive reserve in non-affective first-episode psychosis: contributions of polygenic scores, early clinical features, and environment. Psychological Medicine. 2026;56:e114.
Study Design: Observational cohort analysis of genetic, clinical, and environmental contributors to cognitive reserve.
Sample Size: 174 individuals with non-affective first-episode psychosis.
Key Statistic: The full model explained 17.7% of cognitive-reserve variance; the model without polygenic scores explained 13.5%.
Caveat: The study identifies associations, not a clinical prediction test or proof that genetic scores should guide care by themselves.